

Translate this page into:
A case of pycnodysostosis – Review of classical imaging findings with craniosynostosis – A rare association
*Corresponding author: K. Nadanasadharam, Department of Radiology, Meenakshi Hospital, Thanjavur, Tamil Nadu, India. nadanasadharam912@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nadanasadharam K, Shanmuga Jayanthan S, Yuvaraj N, Shanmuga Hariharan S. A case of pycnodysostosis – Review of classical imaging findings with craniosynostosis – A rare association. Case Rep Clin Radiol. 2024;2:14-8. doi: 10.25259/CRCR_48_2023
Abstract
Pycnodysostosis is a rare skeletal dysplasia, which is characterized by disproportionate short stature, craniofacial abnormalities such as frontal and occipital bossing, small face, beaked nose, hypoplastic mandible, abnormal dentition, and hypoplastic terminal fingers and toes. In addition to these, the hypoplastic lateral end of clavicle, diffuse bone sclerosis, and segmentation anomalies of the spine are also reported. Although classical clinical findings may be present, imaging plays an important role in the diagnosis of this condition by ruling out other osteosclerotic skeletal dysplasias.
Keywords
Skeletal dysplasia
Osteosclerosis
Pycnodysostosis
Cathepsin K

INTRODUCTION
Pycnodysostosis is a rare autosomal recessive skeletal dysplasia, which is due to the deficient activity of the lysosomal protease cathepsin K (CTSK) gene. The disease has equal sex distribution with the incidence of 1–1.7/million birth.[1] Patients with this condition typically have disproportionate short stature, craniofacial abnormalities such as frontal and occipital bossing, hypoplastic mandible, high arched palate, and abnormal dentition. The hands and feet are small with hypoplastic terminal fingers and toes. Osteosclerosis is more obvious in long bone s with delayed closure of cranial sutures. Here in, we present the classical imaging findings of this rare skeletal dysplasia in a 10-year-old boy.
CASE REPORT
A 10-year-old boy born of consanguineous marriage presented with complaints of headache to pediatric OPD. On general examination, the patient height was −103 cm (height for age: <3rd percentile and Z-score was −3). The weight of the patient was 20 kg (weight for age: <3rd percentile and Z-score was −3) and head circumference was 48 cm. On facial examination, there was frontal and occipital bossing with depressed mid face and maxillary hypoplasia. The hard palate showed furrow like depression for the entire length. Soft palate appeared normal. On dental examination, mixed and delayed dentition for the age was noted. Brachydactyly was noted in hands and feet [Figure 1]. Neurological examination was normal without any previous history of developmental delay. His school performance was normal as stated by his parents. Intelligence quotient (IQ) test done elsewhere showed an average IQ score (90–109: WAIS-III). Other systemic examinations were unremarkable. A family history of similar appearance was noted in the late paternal grandfather for which medical records were not available. No evidence of similar abnormality was noted in his elder brother. Routine blood investigations were done. All hematological parameters were within normal limits with hemoglobin – (11.5 g/dL) and renal parameters were normal. Based on the clinical imaging findings, skeletal dysplasia was considered and the patient was referred to radiology for further evaluation.
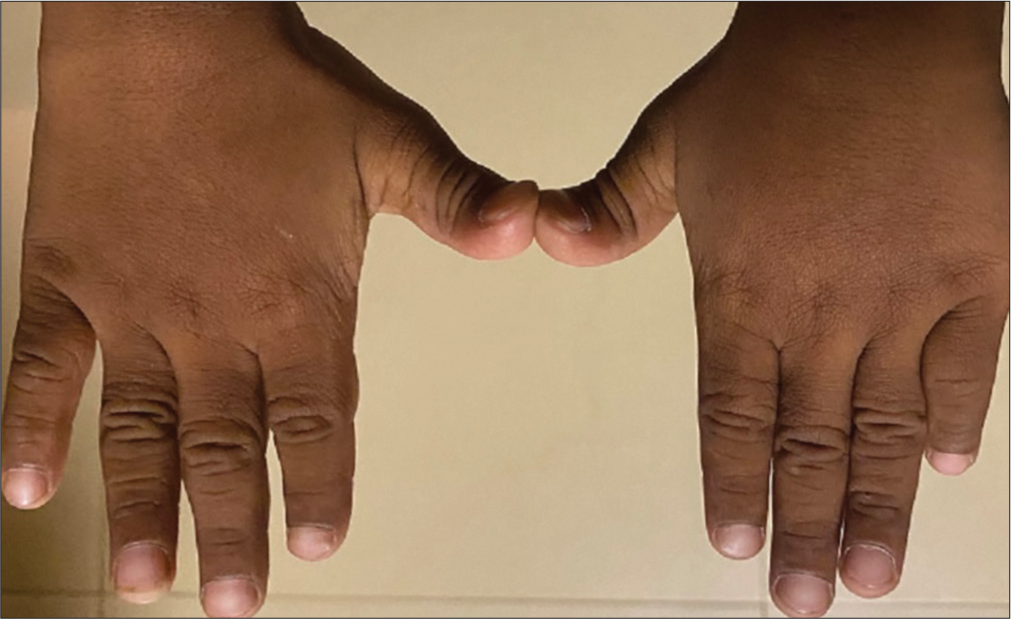
- Clinical image of the patient hands shows a brachydactyly appearance.
On radiological examination, computed tomography brain showed a diffuse increase in skull bone density – s/o Osteosclerosis [Figure 2]. Delayed closure of cranial sutures with open anterior fontanelle, lambdoid, and metopic sutures. Wormian bones were absent in this case [Figure 2]. Sagittal and coronal sutures craniosynostosis with frontal and occipital bossing noted [Figure 2]. Brain parenchyma was normal. No evidence of hydrocephalus or mass lesions in the brain parenchyma [Figure 2]. Hence, headache was attributed to craniosynostosis, which is an extremely rare association. Obtuse mandibular gonial angle with relative prognathism and hypoplastic maxilla with crowded tooth sockets noted [Figure 2].
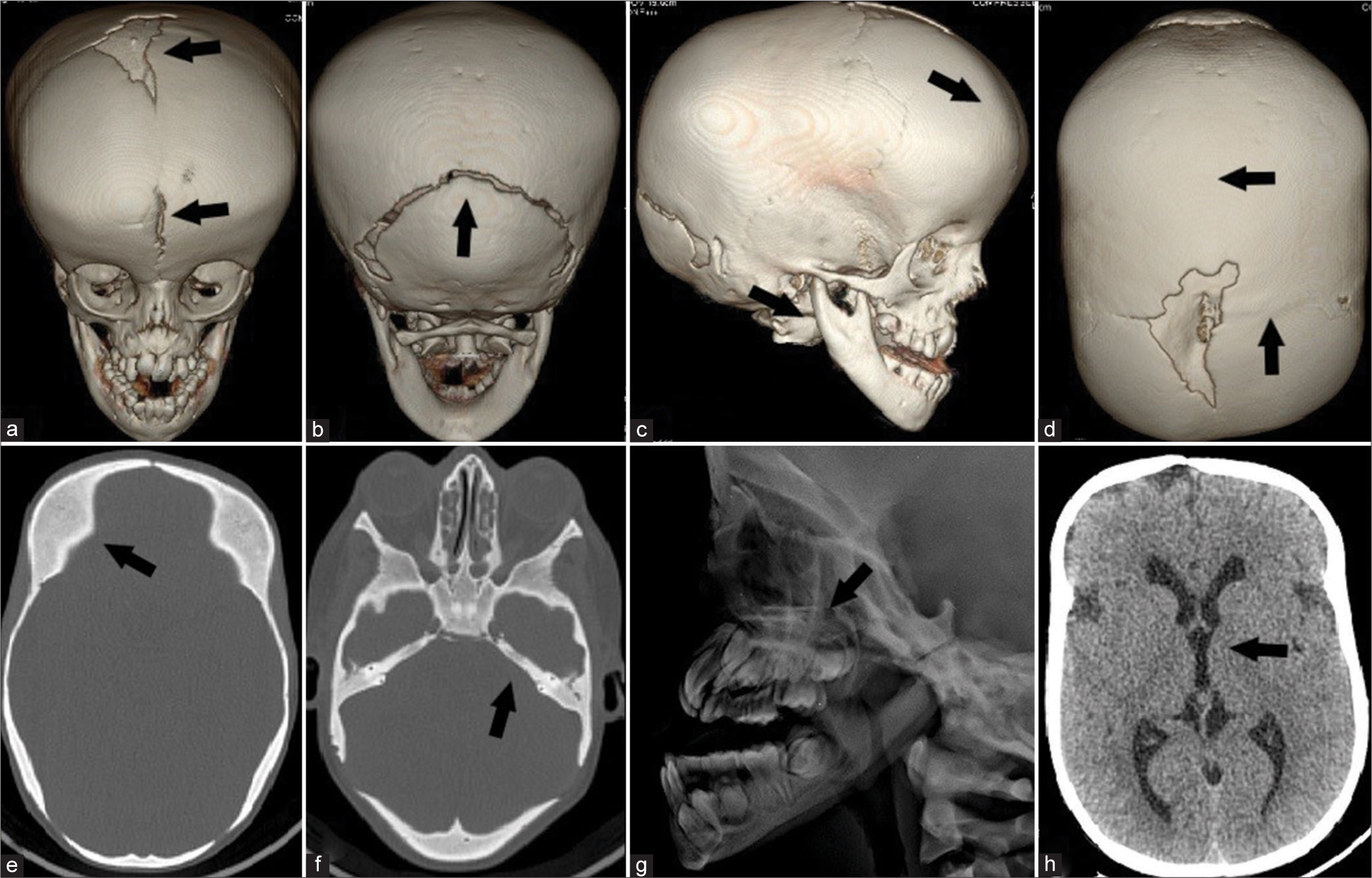
- (a) Volumetric reconstruction image of the skull shows wide anterior fontanelle and persistent open metopic suture. (b) Volumetric reconstruction image of the skull shows a wide open lambdoid suture. No wormian bones are present. (c) Volumetric reconstruction image of the skull shows obtuse gonial angle of the mandible with relative prognathism and froto-occipital bossing also noted. (d) Volumetric reconstruction image of the skull shows craniosynostosis of coronal and sagittal sutures. (e) Computed tomography (CT) brain axial bone window of skull vault shows increased bone density-osteosclerosis. (f) CT Brain axial bone window of skull base shows increased bone density-osteosclerosis. (g) X-ray lateral view shows hypoplastic maxilla with relative prognathism. (h) CT brain axial section shows normal brain parenchyma without any signs of raised increased intracranial pressure or hydrocephalus.
X-ray anterior posterior (AP) view of both hands showed mild medullary expansion of distal radius with remodeled and narrow terminal phalanges, simulating acro-osteolysis [Figure 3]. X-ray AP and lateral view of dorsolumbar spine showed increased bone density. No segmentation anomalies were present [Figure 3]. Normal appearance of clavicle without aplasia/hypoplasia [Figure 3].
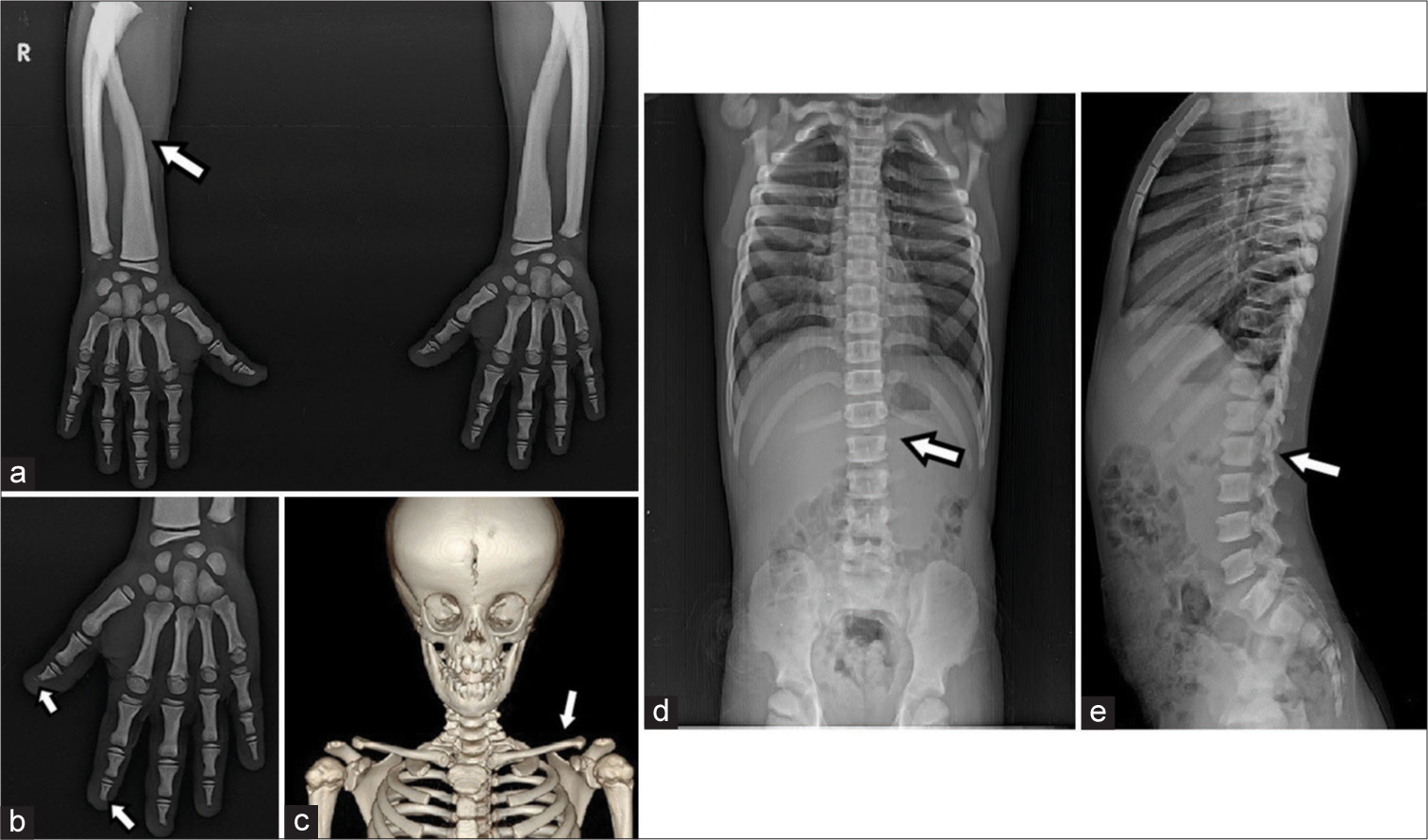
- (a) X-ray anterior posterior (AP) view of both hands shows the mild medullary expansion of distal radius with remodeled and narrow terminal phalanges, simulating acroosteolysis. (b) X-ray left hand shows narrow terminal phalanges with features simulating acroosteolysis. (c) Volumetric reconstruction image shows the normal appearance of both clavicles. (d) X-ray AP view of dorsolumbar spine shows increased bone density. No segmentation anomalies are present. (e) X-ray lateral view of dorsolumbar spine shows increased bone density. No segmentation anomalies are present.
DISCUSSION
Pycnodysostosis is a rare autosomal recessive skeletal dysplasia syndrome. It is due to the deficient activity of the lysosomal protease CTSK gene, which degrades collagen and osteonectin in osteoclasts. 33 Mutations which include non-sense, missense, and stop codon mutations in the CTSK gene, on Chromosome 1q21 have been reported.[2] Deficient activity of the CTSK gene is manifested clinically as osteosclerosis, which leads to increase bone density and stress fractures in weight bearing long bones.[3]
The clinical profile of the patient includes disproportionate short stature, craniofacial deformity, prognathic jaw, short, and stubby fingers/feet.[4] The intraoral features include a groove in the hard palate, overcrowded/persistent primary teeth, and high arched palate.[5]
The radiological findings include failure of cranial sutures to close with a wide anterior fontanelle and numerous wormian bones, predominantly in the lambdoidal region.[6] Frontal and occipital bossing are present. Craniosynostosis may be seen in association with pycnodysostosis but extremely rare, as there are only few cases are described in literature.[7] Obtuse mandibular gonial angle with relative prognathism and hypoplastic maxilla are typical facial features.[4] Acro-osteolysis of distal phalanges of fingers and toes, abnormal dentition, hypoplastic clavicle, and mandible is also seen. Spine anomalies include hyper-lordosis, scoliosis, kyphosis, and block vertebrae.[5]
In some cases, madelung’s deformity, spoon-shaped nails, spool-shaped vertebrae, spondylolysis of C2 and spondylolisthesis of lower lumbar vertebrae, fractures of clavicle and mandible, and deformed rib cage with pectus excavatum are also reported. Shallow and obliquely roofed acetabula and coxa valga may be seen in pelvis.[8]
Other systemic manifestations of this autosomal recessive condition include fragile bones, which might lead to increased risk of fractures. Delayed fracture healing can be a complication as there is incomplete remodeling associated with osteoclast dysfunction. Stridor and laryngomalacia are seen in 20% patients which might lead to obstructive sleep apnea syndrome. Ocular abnormalities include refractive disorders and strabismus, though blindness can occur in association with raised ICT in a few cases. Chest deformities (Kyphosis and narrow chest) can also be seen though in very few cases. Intelligence is typically normal in affected patients, except when associated with brain malformations.[9]
Anemia and splenomegaly are not the features of Pycnodysostosis, as the medullary canal is preserved in this condition.[10,11] Histologically normal cortical bone with decreased osteoblastic and osteoclastic activity is noted. The lamellar bone is sclerotic and contains a large amount of woven bone with a mosaic pattern. Howship’s lacunae are infrequently seen.[12]
The differential diagnosis for Pycnodysostosis includes osteopetrosis, cleidocranial dysplasia, melorheostosis, metaphyseal dysplasia, and osteopathia striata. Pyknodyostosis can be differentiated from osteopetrosis and other differentials by its typical appearance of the skull, mandible and hands.[13] Osteopetrosis is characterized by the involvement of the medullary canal which is spared in pycnodysostosis. Although hypoplastic clavicle can also be seen in cleidocranial dysplasia, the latter is characterized by osteopenia and osteoporosis. The classical imaging findings of the differentials are summarized.
DIFFERENTIAL DIAGNOSIS
The differentials for osteosclerotic bone lesions are mentioned in the Table 1.[10-13]
| Differential diagnosis | Differentiating features |
|---|---|
| Osteopetrosis | Medullary canal is affected Anemia and splenomegaly are present Bone in bone appearance No delayed closure of cranial sutures No phalangeal and clavicle hypoplasia. |
| Cleidocranial dysplasia | Predominantly affects intramembranous ossification Osteopenia and osteoporosis are often seen, but not osteosclerosis Widened sagittal sutures and/or fontanelles Premature fusion of the coronal suture Hypoplasia/aplasia of the lateral clavicle (absent clavicles). |
| Melorheostosis | Periosteal cortical thickening is characteristic Thick undulating ridges of bone, reminiscent of molten wax (dripping wax appearance or flowing candle wax appearance). |
| Metaphyseal dysplasia (Pyles disease) |
Characterized by flaring of the ends of long bones with relative constriction and sclerosis of the diaphysis and mild cranial sclerosis. |
| Osteopathia striata (Voorhoeve disease) |
Radiographically prominent vertical striations predominate in the metaphyses and epiphyses of the long bones (celery stalk metaphysis). |
CONCLUSION
Pycnodysostosis though rare is often diagnosed clinically and with the help of classical imaging findings. Unlike other sclerosing dysplasias, patients with pycnodysostosis usually lead a normal life span; however, hyperplasia of the uvula may rarely lead to hypoventilation and sudden cardiac arrest.
TEACHING POINTS
It is important to be aware of this syndrome as it is very rare and requires a multidisciplinary team for appropriate lifelong management
It is important to be familiar with classical imaging findings which are often diagnostic of this disease
Awareness of the key manifestations and natural history of this inherited disorder will facilitate the prevention and treatment of common complications.
MCQs
-
All are manifestations of pycnodysostosis, except?
Madelung’s deformity
Spoon-shaped nails
Splenomegaly
Spondylolysis
Answer Key: c
-
Mutations in which gene cause pycnodysostosis?
CTSK
CHST3
SOX9
FGFR3
Answer Key: a
-
In pycnodysostosis, the patient’s bone density will be
Reduced
Increased
Not affected
Fluctuated
Answer Key: b
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Clinical and animal research findings in pycnodysostosis and gene mutations of Cathepsin K from 1996 to 2011. Orphanet J Rare Dis. 2011;6:20.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and radiographic features of pycnodysostosis: A case report. J Clin Exp Dent. 2017;9:e1276-81.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical, radiographic, diagnostic and cephalometric features of pycnodysostosis in comparison with Turkish cephalometric norms: A case report. Eur J Dent. 2012;6:454-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pyknodysostosis: Report of a rare case and its dental management. Int J Clin Pediatr Dent. 2020;13:192-5.
- [CrossRef] [PubMed] [Google Scholar]
- The radiology of skeletal disorders (2nd ed). New York: Churchill Livingstone; 1977.
- [Google Scholar]
- Craniosynostosis: A rare complication of pycnodysostosis. Eur J Med Genet. 2010;53:89-92.
- [CrossRef] [PubMed] [Google Scholar]
- Isthmic spondylolisthesis in pycnodysostosis. J Spinal Disord. 1989;2:268-71.
- [CrossRef] [PubMed] [Google Scholar]
- Pycnodysostosis. In: Adam MP, Mirzaa GM, Pagon RA, Wallace SE, Bean LJ, Gripp KW, eds. GeneReviews®. Seattle, WA: University of Washington, Seattle; 2020. p. :1993-2023.
- [Google Scholar]
- Sclerosing bone dysplasias--a target-site approach. Skeletal Radiol. 1991;20:561-83.
- [CrossRef] [PubMed] [Google Scholar]
- Cathepsin K inhibitors for osteoporosis: Biology, potential clinical utility, and lessons learned. Endocr Rev. 2017;38:325-50.
- [CrossRef] [PubMed] [Google Scholar]




