

Translate this page into:
In a fetus’ “CHAOS” there is no cosmos, in this disorder exists only one order
*Corresponding author: Vivek Gupta, Department of Radiology, Orange Clinic, Palghar, Maharashtra, India. drvivekradiology@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta V, Bhandari K, Shetty SR. In a fetus’ “CHAOS” there is no cosmos, in this disorder exists only one order. Case Rep Clin Radiol. 2025;3:71-4. doi: 10.25259/CRCR_167_2023
Abstract
Congenital high airway obstruction syndrome (CHAOS) is a partial or complete obstruction of the fetal upper airways and is an extremely rare entity. The most common cause of CHAOS is tracheal or laryngeal atresia. Laryngeal agenesis, laryngeal webs or cysts, and even subglottic stenosis can be rare causes. We present the rare case of a large cervical teratoma impinging on the upper airways of a fetus and causing CHAOS.
Keywords
CHAOS
Teratoma
Ultrasound
Antenatal

INTRODUCTION
Congenital high airway obstruction syndrome (CHAOS) is an extremely uncommon condition which occurs in fetuses classically due to laryngeal atresia.[1,2] It can rarely also be caused due to a mass impinging on the airway and causing upper airway obstruction. Teratomas are relatively common in the sacrococcygeal region but occasionally also reported in the cervical region. Unusually, a cervical mass like teratoma can obstruct the upper airway, particularly the larger ones. This can lead to development of the same chest pathology as seen in laryngeal atresia. Antenatal ultrasound is the investigation of choice in diagnosis of CHAOS. The classic ultrasound picture is that of bilateral expanded hyperechoic lungs. Because prognosis is poor in such cases, ultrasound diagnosis in antenatal period is paramount. There have been advances in fetal interventions particularly the advent of the EXIT (ex-utero intrapartum treatment) procedure which has been advocated in aiding management of such airway compression cases where available.
CASE REPORT
A 19-year-old female patient was referred to our clinic for a routine second-trimester ultrasound. She was primigravida at 22 weeks at the time of presentation. No significant clinical history to suggest genetic or familial disorders was elicited.This was her first ultrasound in the pregnancy.
Ultrasound [Figure 1] revealed a single live intrauterine fetus of 22 weeks with a large well-defined exophytic mass protruding anterolaterally from the neck. It measured roughly 52 mm × 46 mm and comprised solid as well cystic components = honeycomb appearance. On color Doppler, vascularity was appreciated in some of the solid areas. No calcifications were seen. Besides the exophytic component protruding externally from the fetal neck, the mass extended internally involving the deep cervical tissues as well as impinging upon and obstructing the fetal upper airway at the cervical level. The airway was distal to the obstruction by the mass and appeared mildly dilated. The fetal lungs were hyperexpanded and hyperechoic symmetrically with flattening of the diaphragm. This appearance was classic of congenital high airway obstruction syndrome (CHAOS). Associated with CHAOS, fetal ascites were also observed, indicating evolving hydrops. Moderate polyhydramnios was noted.

- (a) Ultrasound image (sagittal) of the fetal chest depicting the cervical teratoma/mass (blue arrow) obstrcuting the airway leading to bilateral symmetrically expanded hyperechoic lungs (orange arrows), (b) sagittal view of the teratoma (blue arrow) in cervical region, (c) the heart (green arrow) is compressed by the hyperechoic expanded lungs (orange arrows) in axial view.
The patient was counseled regarding the unfavorable outcome for the fetus. The benefits and limitations of the EXIT procedure were also explained to her. She opted for termination of pregnancy. Histopathology evaluation of the mass confirmed it to be a teratoma [Figures 2 and 3].

- Gross specimen of abortus with the large cervical mass.
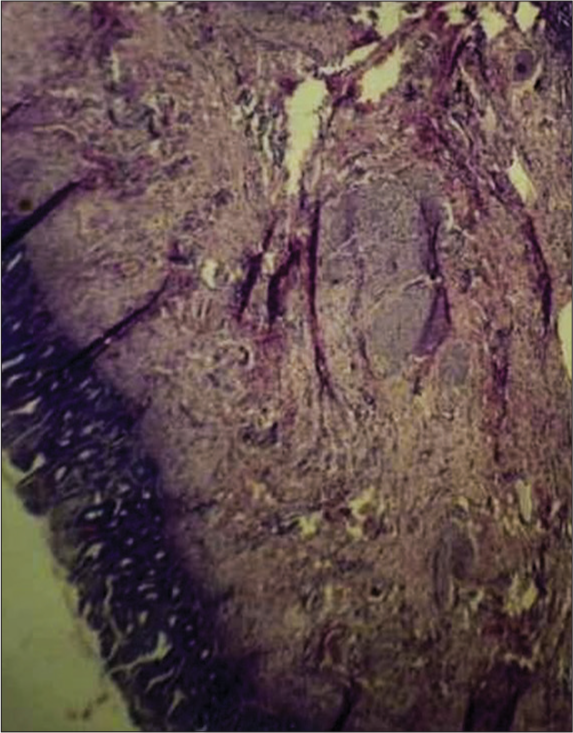
- Microscopic slide from histopathology of the mass confirming teratoma (Hematoxylin & Eosin stain, 20X).
DISCUSSION
Teratomas are tumors derived from all three germ cell layers, ectoderm, mesoderm, and endoderm, and are therefore comprised of components of all three. They are most frequently reported in the sacrococcygeal region. Cervical teratomas are the second most frequent perinatal germ cell tumor, with an estimated birth incidence of 1/20,000–40,000 live births.[3,4] Being mostly benign, they can be resected at birth. However, in rare cases, their location might be responsible for causing in utero airway obstruction and distortion in the fetus.[5] Giant teratomas can compress the hypopharynx as well as the esophagus, impairing the swallowing of fluid by the fetus and resulting in polyhydramnios. They are typically solid-cystic vascular masses on ultrasound, with calcifications identified in about 50% of cases.
When the trachea-bronchial tree gets obstructed, accumulation of lung fluids leads to elevation of intratracheal pressure and enlargement of lungs in CHAOS. Eventually, reduced venous return, impaired cardiovascular function, and hydrops follow. Although laryngeal atresia is the most common cause of CHAOS, it may also be caused by obstructing oropharyngeal tumors and even a double aortic arch.[6] Characteristic findings of CHAOS on antenatal ultrasound include bilateral large hyperechoic lungs, dilated tracheobronchial tree, small and compressed centrally placed heart, flattened or inverted diaphragm, and ascites.[7] Antenatal ultrasound is therefore of paramount significance in the diagnosis of this rare condition so that timely decisions regarding management can be taken. The cause of primary CHAOS is unknown and is sporadic. CHAOS is associated mostly with Fraser’s syndrome, although it has been linked with the short-rib polydactyly syndrome, Shprintzen-Goldberg Omphalocele syndrome, and vertebral anorectal cardiac tracheoesophageal renal limb (VACTERL) association as well as some chromosomal anomalies.
Fetal magnetic resonance imaging can be suggested which can confirm the findings and aid in management particularly if a surgical intervention is being planned. It is considered more effective in defining the exact level of obstruction.
The EXIT procedure is a specialized surgical procedure to manage babies with airway compromise. Originally devised to reverse temporary tracheal occlusion in cases of fetal surgery for severe congenital diaphragmatic hernia, EXIT procedures have benefited the management of other causes of airway compromise such as giant cervical teratomas.[8] It allows for safe delivery and the avoidance of airway obstruction. During the procedure, the head, neck, and shoulders of the fetus are delivered through a hysterotomy, thereby maintaining uterine volume and minimizing uterine contractions. In addition to the time needed for surgical resection, this provides adequate time for techniques necessary to secure the airway, including surfactant administration, direct laryngoscopy, bronchoscopy, and tracheostomy procedures. The EXIT procedure provides up to 1 h of uteroplacental support in fetal patients with giant cervical teratomas.[9]
Only about 2.3–9.3% of all teratomas are in the cervical region with an incidence of 1 in 20,000–40,000 live births.[10] Of these cases, cervical teratomas associated with CHAOS are even fewer and have been rarely reported.
DIFFERENTIAL DIAGNOSIS
Classical CHAOS is described as caused by laryngeal atresia where the obstruction lies in the larynx seen as “V”-shaped narrowing of the airway. Our case is, therefore, unusual where the cause of obstruction leading to CHAOS is a neck mass.
Bilateral CPAM type III, although it may simulate CHAOS, both bilateral CPAM and type III CPAM lesions are uncommon and would be quite rare in combination, affecting a major part of both lungs.
Vascular rings such as double aortic arch, may cause airway obstruction when they are tight. Doppler can help identify these aberrant vessels.
Some differentials of fetal neck masses are lymphangiomas, hemangiomas, teratomas, goiter, and neuroblastoma, although they may not necessarily cause airway obstruction unless they are large and firm masses.
CONCLUSION
CHAOS is a very rare condition with adverse outcome but can be diagnosed by antenatal ultrasound. Cervical masses like teratoma can rarely obstruct the airways and cause CHAOS. CHAOS has a classical ultrasound picture of the chest which should alert the examiner and timely diagnosis should be achieved. Antenatal interventions have been developed for fetuses with airway compression like the EXIT procedure which can be offered where available if patient is willing to continue the pregnancy.
TEACHING POINTS
CHAOS is a very rare condition with unfavorable perinatal outcomes, although it can be diagnosed easily on antenatal ultrasound by its characteristic features including bilateral hyperexpanded fetal lungs.
Although all conditions that cause compromise or obstruction of airways in the antenatal period have a bad prognosis, they can be offered procedures such as EXIT which are known to improve and benefit perinatal outcomes in such patients.
MCQs
-
What are the characteristic ultrasound findings in CHAOS?
Bilateral echogenic lungs
Flattening of diaphragm
Bilateral hyperexpanded lungs
All of the above
Answer Key: d
-
What is the most common location for an antenatally identified teratoma
Cervical
Thoracic
Sacrococcygeal
None of the above
Answer Key: c
-
With what syndrome is CHAOS most frequently associated with?
Holt-Oram
Tuberous sclerosis
Fraser’s
Down’s
Answer Key: c
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Predicting the severity of congenital high airway obstruction syndrome. J Pediatr Surg. 2010;45:1633-9.
- [CrossRef] [PubMed] [Google Scholar]
- Fetal tracheolaryngeal airway obstruction: Prenatal evaluation by sonography and MRI. Pediatr Radiol. 2010;40:1800-5.
- [CrossRef] [PubMed] [Google Scholar]
- Ex utero intrapartum treatment in the management of giant cervical teratomas. J Pediatr Surg. 2012;47:1208-16.
- [CrossRef] [PubMed] [Google Scholar]
- Prenatal MRI evaluation of giant neck masses in preparation for the fetal exit procedure. Am J Perinatol. 1998;15:253-7.
- [CrossRef] [PubMed] [Google Scholar]
- Management of fetal teratomas. Pediatr Surg Int. 2016;32:635-47.
- [CrossRef] [PubMed] [Google Scholar]
- A practical approach to fetal chest masses. Ultrasound Q. 2006;22:177-94.
- [CrossRef] [PubMed] [Google Scholar]
- Prenatal diagnosis of congenital high airway obstruction syndrome (CHAOS) Five case report. Med Ultrason. 2015;17:115-8.
- [CrossRef] [PubMed] [Google Scholar]
- The EXIT procedure: Experience and outcome in 31 cases. J Pediatr Surg. 2002;37:418-26.
- [CrossRef] [PubMed] [Google Scholar]
- A huge immature cervical teratoma; antenatal diagnosis, and its management-an unusual entity. J Clin Neonatol. 2013;2:42-5.
- [CrossRef] [PubMed] [Google Scholar]
- A case of cervical teratoma in an infant. Indian J Otolaryngol Head Neck Surg. 2022;74:6519-23.
- [CrossRef] [PubMed] [Google Scholar]




