

Translate this page into:
Tricuspid valve metastasis in osteosarcoma, paving way through iliofemoral vessels – An unusual presentation of a usual diagnosis
*Corresponding author: Dr. Jyoti Gupta, Assistant Professor, Department of Radiodiagnosis and interventional Radiology, VMMC and Safdarjung Hospital, New Delhi, India. jyotigupta99@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bagchi N, Gupta J, Chauhan BS, Bhayana A. Tricuspid valve metastasis in osteosarcoma, paving way through iliofemoral vessels – An unusual presentation of a usual diagnosis. Case Rep Clin Radiol. 2024;2:11-3. doi: 10.25259/CRCR_31_2023
Abstract
Hematogenous spread of osteosarcoma is a common knowledge, with frequent metastases to lungs and bones. Cardiac involvement is rare finding, most of them depicting contiguous cardiac extension through vessels into the right atrium. Tricuspid metastases are rare. We encountered one such rare case of femur osteosarcoma with multiorgan metastasis including systemic veins, cardiac chambers, and tricuspid valve involvement which presented as diagnostic dilemma. Early detection was crucial for further management and prognostication of patient.
Keywords
Metastatic osteosarcoma
Intravascular metastases
Tricuspid valve metastases

INTRODUCTION
Osteosarcoma is a malignant bone tumor with bimodal age distribution, frequently involving long bones, in the second and third decades of life.[1] Hematogenous spread of osteosarcoma is common to the lungs and bones. After doing a thorough literature search, we observed an extreme paucity of reports on the primary or secondary cardiac involvement in osteosarcoma, with nearly all the cases reported in western literature. To the best of our knowledge, no case has been reported on such an association in the Indian literature so far.[2,3] Moreover, imaging findings of cardiovascular involvement are often subtle and are most likely missed, if superadded by the absence of clinical complaints, leading to fatal consequences. Early recognition can thus help in accurate disease staging and future prognostication.
CASE REPORT
A 16-year-old male patient with a past history of above knee amputation for chondroblastic osteosarcoma of the left distal femur presented to a tertiary hospital with complaints of pain over the amputated leg. He also received six cycles of adjuvant chemotherapy. Physical examination was unremarkable with a healthy stump and no other systemic complains. Laboratory examination showed normocytic normochromic anemia and mild thrombocytopenia.
Left hemipelvis radiograph [Figure 1a] including the amputated left leg showed patchy, well-defined, coarse, and curvilinear tubular radiopacities with osseous matrix, along the left hemipelvis and left inguinal region. Furthermore, few discrete rounds to oval nodal deposits with osseous matrix were seen along these tubular radiopacities. On ultrasound, left sided iliofemoral veins and infrarenal inferior vena cava (IVC) appeared grossly dilated, showing completely occluding intraluminal echogenic thrombus with large calcific foci [Figure 1b and c]. The intrahepatic part of IVC showed a partially occluding thrombus [Figure 2]. Hepatic veins and both renal veins were unremarkable. Chest X-ray revealed multiple random radiopacities in bilateral lung fields with calcifications. On transthoracic cardiac ultrasound, a small isolated echogenic mass was seen attached to tricuspid leaflet, protruding into the right ventricle [Figure 3a]. This was confirmed on subsequent contrast-enhanced cardiac magnetic resonance imaging (MRI) [Figure 3b] which depicted heterogeneous post-contrast enhancement. MRI further revealed a heterogeneously enhancing lesion within suprahepatic IVC, extending through cavoatrial junction into right atrium suggestive of tumor thrombus and disease progression [Figure 3b and c]. A similar morphology tumor thrombus was additionally seen in the right main pulmonary artery [Figure 3d] extending into its upper segmental branch. Multiple intrapulmonary metastases were observed as well. The patient was referred for chemoradiotherapy in view of extensive metastases.
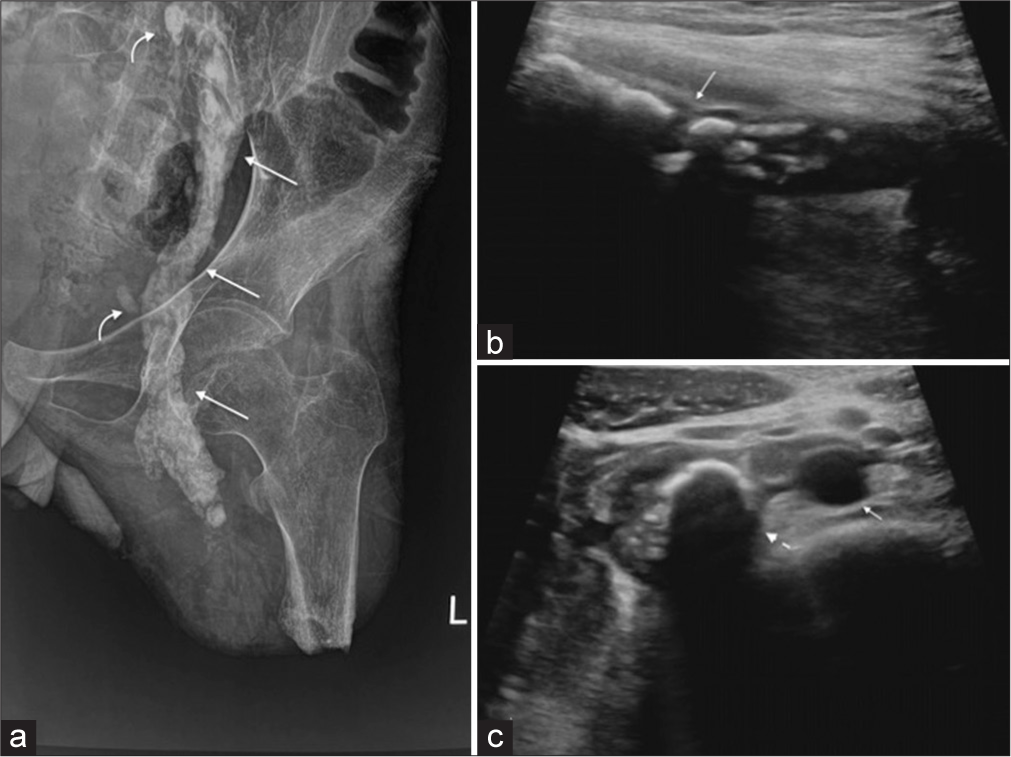
- (a) X-ray left hemipelvis shows curvilinear tubular radio-opacities along the course of iliofemoral vessels (straight arrows) with adjacent small oval radio-opacities (curved arrows). (b and c) Targetted ultrasound of the vessels shows intraluminal thrombus with chunky foci of calcification and posterior acoustic shadowing with iliofemoral vessels (solid arrow in b) and infrahepatic Ic (Dashed arrow). Adjacent aorta (solid small arrow in c) shows anechoeic lumen.
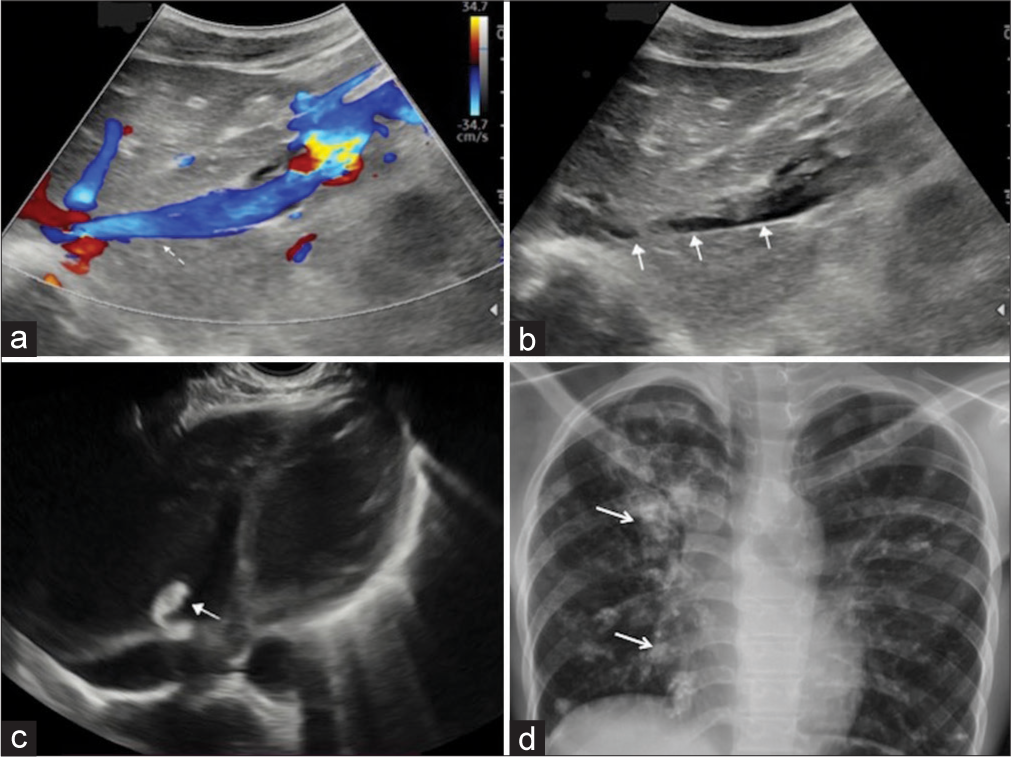
- Color Doppler (a and b) mode ultrasound (b) of intrahepatic inferior vena cava shows partially occluding thrombus (solid arrows) with partial color flow (dashed arrow). Transthoracic basal view of cardiac chambers shows a small echogenic thrombus (solid arrow) along the tricuspid valve with clear right ventricle (c). Chest X-ray PA view (d) shows multiple randon ill-defined high-density radio-opaque masses (arrows) with calcification in both lung fields.
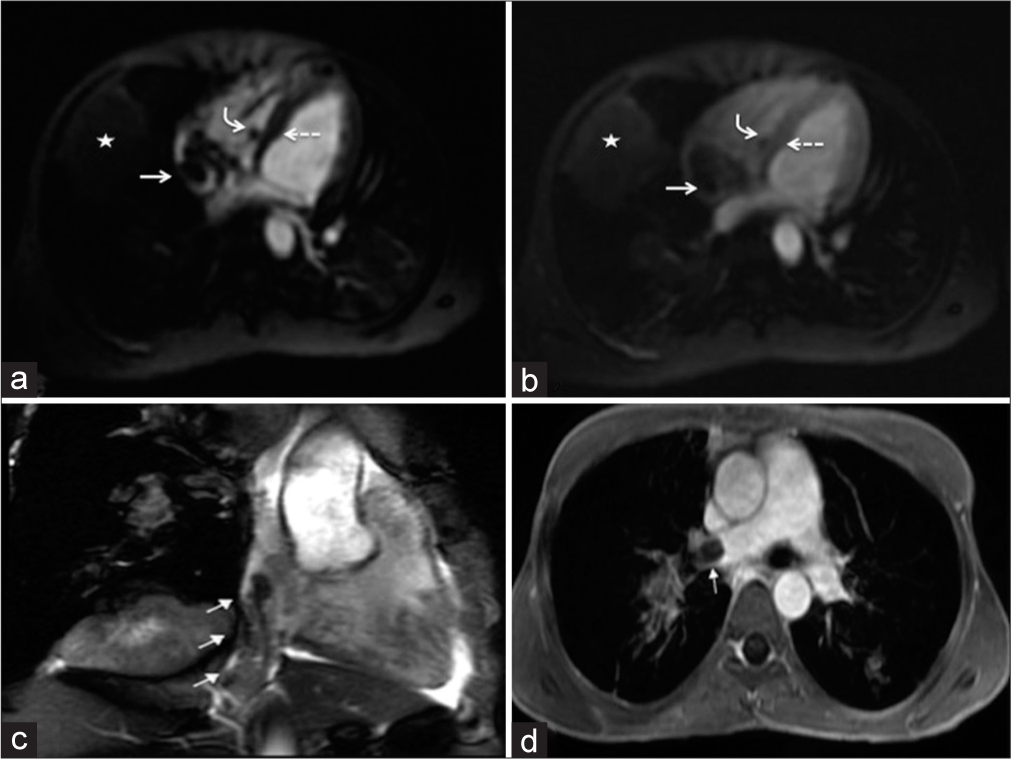
- Horizontal long axis four chamber early blood pool phase perfusion cardiac magnetic resonance imaging (MRI) (a) shows the thrombus attached to tricuspid valve (curved arrow), intraluminal thrombus in right atrium (straight arrow) and right lung parenchymal mass (star) with mild heterogeneous enhancement of the tumor thrombi as well as right lung mass on subsequent perfusion phase (b) which is however less as compared to the enhancement of adjacent myocardium (dashed arrow). Vertical long axis right-sided 3 chamber view on MRI (c) shows tumor extending from suprahepatic inferior vena cava to right atrium (short solid arrows). Axial 10 min delayed thrive post-contrast MRI shows (d) heterogeneous signal intensity thrombus (arrow) in the right pulmonary artery.
DISCUSSION
Osteosarcoma is a malignant bone tumor which commonly metastasizes to lungs and bones. Although hematogenous metastasis is common, osteosarcoma very rarely metastasizes to heart. Very few cases have been reported of metastases to the right ventricle, most of them in the right ventricular outflow tract, pulmonary arteries, or pulmonary veins. One case of metastatic osteosarcoma with tumor mass attached to tricuspid valve[1] was previously reported, similar to our case. Although, some of these cases were diagnosed during routine investigation for severe cardiac failure, most of them were diagnosed at autopsy.[4] In an autopsy review of osteosarcoma, nearly 20% of cases showed cardiac metastases.[5] Such cases can be challenging for diagnosis in patients antemortem, especially with no clinical symptoms.
Important learning from our case report is that in a follow-up case of proven osteosarcoma, careful examination of the radiographs should be done, as a vascular tumor thrombus is often mistaken for nodal metastasis, which can be present simultaneously, as was in our case. This can be avoided by color Doppler correlation of the affected limb and abdomen. Cardiac MRI can further determine the exact intracardiac and intravascular tumor thrombus extent in cases, picked up by ultrasound. Moreover, it is of utmost important to differentiate tumor thrombus in veins and pulmonary arteries from a bland thrombus, which changes the management plan. Unlike a bland thrombus, tumor thrombus mimics the characteristics of the primary tumor in enhancement and mineralization as depicted in our case.[6]
CONCLUSION
Multiorgan metastatic osteosarcoma with cardiovascular involvement is seldom reported. Key to diagnosis is radiographic recognition of intravascular tumoral metastases followed by thorough scanning of entire circulation. Early detection of cardiovascular metastasis plays a pivotal role in accurate staging and guiding the clinicians in appropriate management and prognostication of patients.
TEACHING POINTS
High index of suspicion should be there for intravascular metastases in cases of unusual clinical presentation of osteosarcoma patients.
Multimodality multidisciplinary approach is necessary for diagnosis and management of the patients.
Rare possibility of intracardiac metastases should be kept in mind and CEMRI plays important role in differentiating bland thrombus from tumoral thrombus.
MCQs
-
Differentials for a curvillinear calcification in pelvis inculde, all except-
Lymph nodal metastases
Intravascular metastases
Rim calcification of solid lesions
None of the above
Answer Key: d
-
The key difference between bland thrombus and tumor thrombus is
Size
Vascularity
Calcification
All of the above
Answer Key: b
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Tumour on the tricuspid valve: Metastatic osteosarcoma and the heart. Can J Cardiol. 2005;21:63-7.
- [Google Scholar]
- Osteosarcoma metastases with direct cardiac invasion: A case report and review of the pediatric literature. J Pediatr Hematol Oncol. 2017;39:188-93.
- [CrossRef] [PubMed] [Google Scholar]
- A primary cardiac osteosarcoma: Case report and review of the literature. J Cardiol Cases. 2013;7:29-33.
- [CrossRef] [PubMed] [Google Scholar]
- Right ventricular obstruction secondary to intracardiac metastatic osteosarcoma. Clin Cardiol. 1980;3:200-3.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular involvement by osteosarcoma: an analysis of 20 patients. Pediatr Radiol. 2016;46:21-33.
- [CrossRef] [PubMed] [Google Scholar]




