

Translate this page into:
Infantile inguinal hernia complicated with ileoileal intussusception

*Corresponding author: Khushboo Tekriwal, Department of Radiology, Seth GS Medical College and King Edward Memorial (KEM) Hospital, Mumbai, Maharashtra, India. khushbootekriwal300995@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Shetty H, Thakkar H, Tekriwal K, Bhoir AA. Infantile inguinal hernia complicated with ileoileal intussusception. Case Rep Clin Radiol. doi: 10.25259/CRCR_156_2023
Abstract
Indirect inguinal hernias occur due to patent processus vaginalis. One-third of cases present before 6 months of age. Despite being one of the most performed surgeries, inguinal hernia repair can be complicated due to unusual contents in the hernia sac. One commonly encountered unusual structure is the vermiform appendix. Less commonly, epiploic appendages, ovaries, uterus, urinary bladder, and fallopian tubes have also been encountered in the hernia sac. Intussusception as a content of the hernial sac is rare. We present a case of an indirect inguinal hernia complicated by ileoileal intussusception causing acute intestinal obstruction in a 2-month-old infant. To our knowledge, no such case has been described in the literature in the pediatric population.
Keywords
Indirect inguinal hernia
Intussusception
Complication
Bowel obstruction

INTRODUCTION
Indirect inguinal hernia is among the most common hernias in pediatric patients. Small bowel loops are the most common contents in the hernia sac. It is common to find unusual contents in the hernia sac, which can complicate the surgeries. Hence, imaging should be performed at the earliest to characterize the herniated content, viability, and possible complications.
CASE REPORT
A 2-month-old baby boy was brought to the pediatric emergency department with complaints of left scrotal swelling for 12 h associated with inconsolable crying. The baby had not passed stools since then. On abdominal examination, his abdomen was distended and tense. However, there was no guarding. On local scrotal examination [Figure 1], a firm tense swelling was noted on the left side. An emergency ultrasonogram was performed.

- Clinical photographs of the inguinoscrotal region of a 2-month-old baby boy with left inguinoscrotal hernia complicated by ileoileal intussusception show (a) Pre-reduction photograph: Groin swelling with signs of inflammation (black arrow) and penile tumescence on the left side. (b) Post-reduction photograph: Complete resolution of groin swelling and relief of penile engorgement. Images have been taken with patient’s consent. This case report has been approved for publication by the Institutional Ethics Committee at Seth GS medical college and KEM hospital, Mumbai. Number EC/CR-07/2023, dated 12/12/2023.
An ileal loop was seen herniating into the left inguinal canal up to the upper pole of the left testis through the enlarged (6 mm) deep inguinal ring on the ultrasonogram [Figure 2]. Another ileal loop was seen telescoping into this loop for a length of 1.8 cm, giving bowel within bowel appearance or target sign suggesting associated ileoileal intussusception. The neck of the hernial sac served as the lead point of this intussusception. The herniated bowel walls were thick, edematous, and congested, with slightly increased vascularity. The left testis and epididymis were also congested and bulky, secondary to spermatic cord compression due to the hernial sac. A mild hydrocele with septa was seen in the sac. The small bowel loops proximal to the neck of the hernial sac were dilated and showed to-and-fro peristaltic movements. The right testis was displaced high up into the inguinal canal.
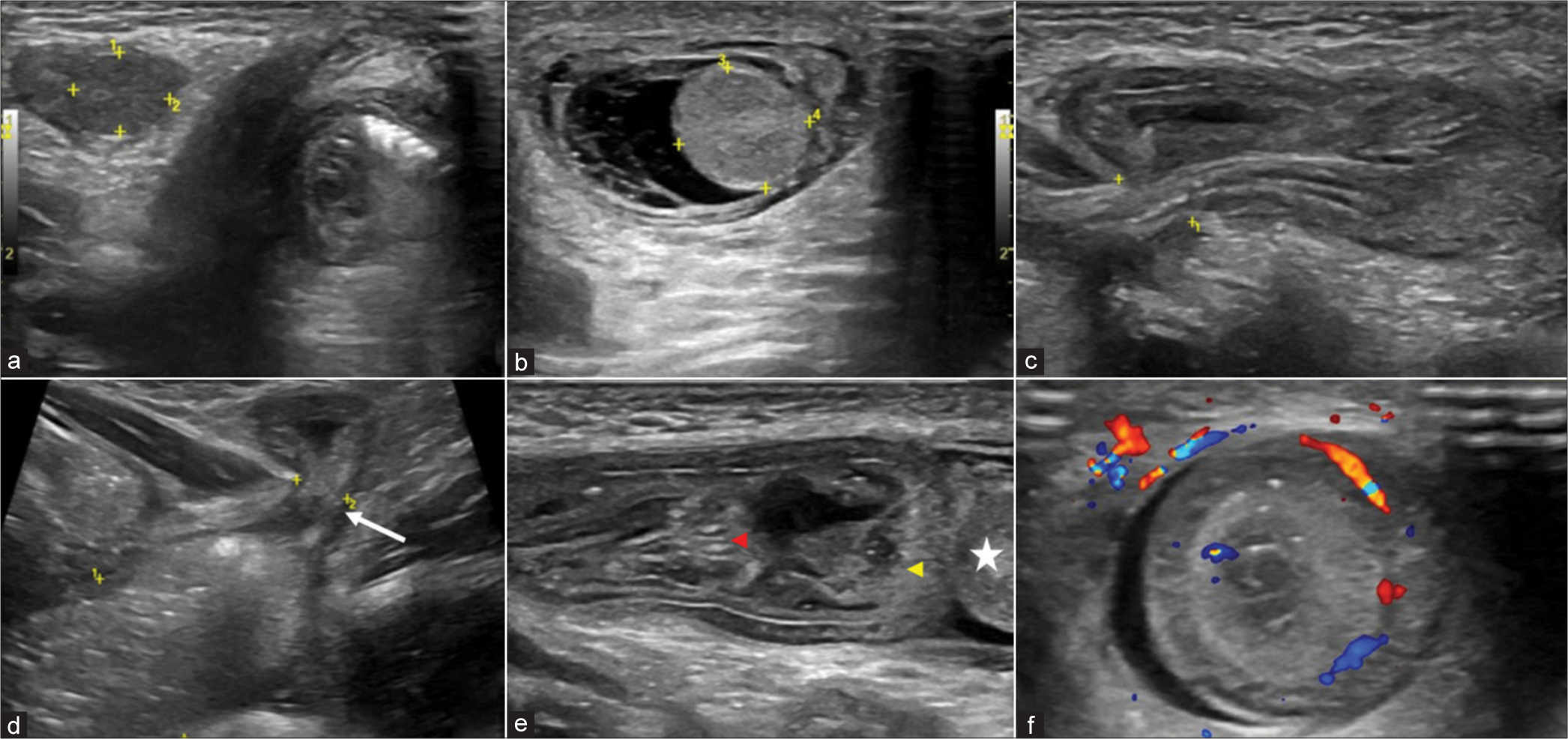
- An ultrasonogram of the inguinoscrotal region of a 2-month-old baby boy with left inguinoscrotal swelling using a linear high-frequency transducer shows (a) a normal-sized testis in the right inguinal canal with normal echogenicity, (b) bulky echogenic testis in the left scrotal sac with adjacent mild hydrocele, (c) shows herniating small bowel loop through the enlarged left deep inguinal ring, (d) shows dilated small bowel loops proximal to the neck of the hernia with the transition at the neck (white arrow), (e) shows telescoping of another small bowel loop (red arrowhead) for a length of 1.8 cm into the herniated bowel loop (yellow arrowhead) reaching up to the testis (white star), and (f) transverse section of the herniated bowel loops shows a characteristic bowel within bowel appearance or target sign intussusception.
The ultrasonogram findings were immediately conveyed to the treating pediatricians. Manual reduction of the intussusception and hernia was attempted. An hour later, a repeat ultrasound examination showed persistent ileoileal intussusception with a similar length of the intussusceptum. The reduction was attempted again under sedation to achieve minimal abdominal muscle tension. The swelling over the left scrotal region subsided with a reduction of the contents, and the baby started passing copious amounts of stool. The repeat ultrasonogram [Figure 3] showed a complete reduction of the herniated bowel loops and intussusceptum, with the associated small bowel obstruction settled. However, the left testis and epididymis were bulky and edematous, and the left deep inguinal ring was persistently enlarged. The right testis relocated to the scrotum.
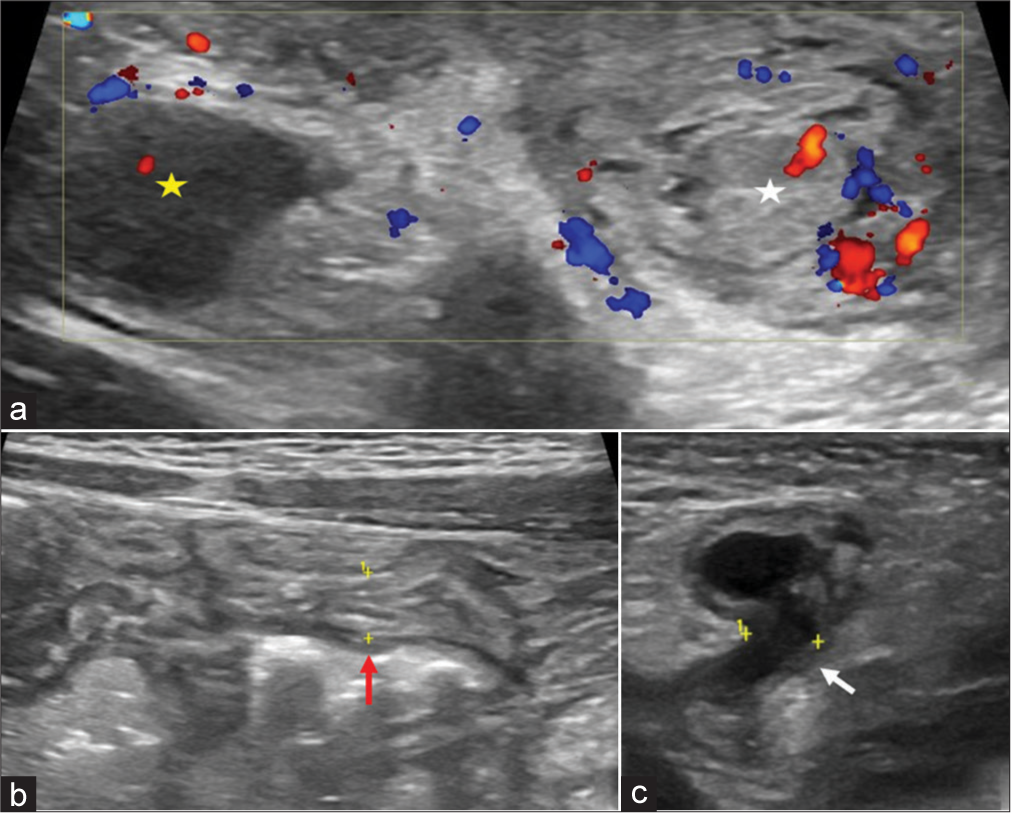
- An ultrasonogram of the inguinoscrotal region of a 2-month-old baby boy performed after the reduction of herniated small bowel intussusception using a linear high-frequency transducer shows (a) a normalized testis in the right scrotal sac with normal echogenicity (yellow star) and a hyperechoic testis and epididymis in the left scrotal sac (white star), (b) normal caliber of small bowel loops (red arrow), and (c) persistently enlarged left deep inguinal ring (white arrow) with mild free fluid tracking into the inguinal canal, no bowel loop is seen herniating through the defect.
The baby underwent an elective laparoscopic bilateral hernioplasty the following day with an uneventful postoperative period. Four days later, a follow-up sonogram was performed [Figure 4], which revealed the resolution of edema or congestion of the left testis and epididymis. There was minimal communicating hydrocele on both sides, with an enlarged right deep inguinal ring measuring 5 mm. The baby was discharged the next day and was followed up on an outpatient department basis. Six months later, a repeat sonogram showed normal deep inguinal rings with no detectable communication of the peritoneum with the inguinal region. This case report has been approved for publication by the Institutional Ethics Committee at Seth GS medical college and KEM hospital, Mumbai. Number EC/ CR-07/2023, dated 12/12/2023.
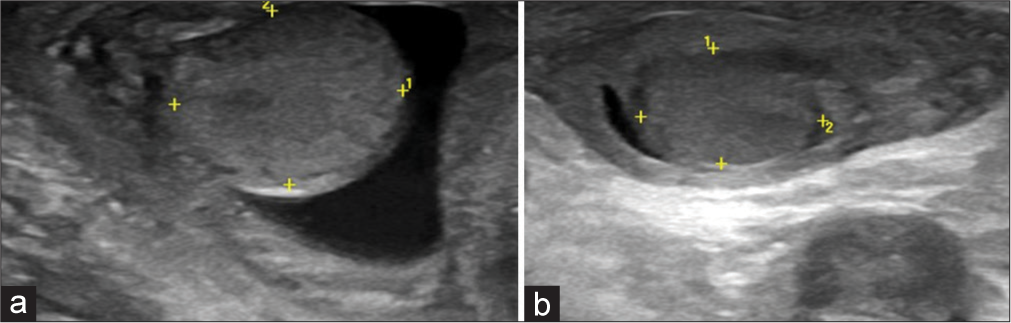
- A follow-up ultrasonogram 4 days after the reduction of the left inguinal hernia shows (a) right testis and (b) left testis with normalization of echogenicity of the left testis.
DISCUSSION
The processus vaginalis is an evagination of the parietal peritoneum, accompanied by the testis in males or the round ligament of the uterus in females through the deep ring of the inguinal canal toward the scrotum or labia majora, respectively.[1] Pediatric inguinal hernias are caused due to herniation of the abdominal contents through a patent processus vaginalis with a male preponderance of 6:1.[2]
Although inguinal hernia repair is a commonly performed surgery, it can be complicated due to unusual contents in the hernia sac.[3] One commonly encountered unusual structure is the vermiform appendix. Less commonly, epiploic appendages, ovaries, uterus, urinary bladder, and fallopian tubes have also been encountered in the hernia sac.[4,5] Intussusception as a content of the hernial sac is rare. It has predominantly been reported in adults as the content of internal paraduodenal hernias, umbilical hernias, and post-abdominal surgeries where the hernia served as a lead point for intussusception.[6-9] Only a few cases of inguinal hernias complicated with intussusception have been described in the literature, but none have been reported in the pediatric population. Gopal and Solomon described an inguinal hernia complicated by ileoileal intussusception with an ileal tumor serving as the lead point and a large hematocele within the sac in a middle-aged man.[3]
Intestinal necrosis and testicular ischemia are critical complications of the inguinal hernia complicated with intussusception. Duration of the onset of symptoms and hematochezia are the ominous indicators of intestinal necrosis for patients who failed non-surgical reduction.[10] Ultrasound with color Doppler is the modality of choice for characterizing and accessing the viability of the herniated content and keeping an eye on possible testicular ischemia. Ultrasound is also used to look for contralateral involvement due to the high incidence of contralateral patent processus vaginalis (50% in males and 90% in females). Few ultrasound criteria are laid off to diagnose a contralateral patent processus vaginalis. The presence of hydrocele within the inguinal canal is considered a definitive finding or an opening >4 mm at the deep inguinal ring is considered positive.[11,12]
CONCLUSION
Ultrasound with color Doppler should be performed at the earliest to assess the viability of the herniated content and keep an eye on possible complications such as volvulus or intussusception of the herniated bowel loop or testicular ischemia.
TEACHING POINTS
Early diagnosis of inguinal hernia is essential as the herniated contents can cause spermatic cord compression, leading to testicular ischemia.
Careful evaluation of the herniated bowel loops is crucial as they can be complicated with volvulus or intussusception and can lead to necrosis and perforation of the bowel loop due to vascular compromise if not reduced on time.
An obstructed inguinal hernia is a known emergency, as it can lead to bowel ischemia and perforation if not treated on time. Hence, prompt communication with the treating doctors is crucial.
The contralateral inguinal ring assessment is also crucial due to the high incidence of patent contralateral processus vaginalis.
MCQs
-
Which of the following is a form of internal hernia?
Inguinal hernia
Richter hernia
Para duodenal hernia
Incisional hernia
Answer Key: c
-
What is the most common type of intussusception?
Ileoileal
Ileocolic
Colocolic
Gastric
Answer Key: b
-
Which of the following is a false statement?
Indirect inguinal hernia occurs due to the persistence of processus vaginalis
About one-third of indirect inguinal hernias are present during infancy
Direct inguinal hernias are medial to the inferior epigastric artery
About one-third of direct inguinal hernias presents before 6 months of age
Answer Key: d
Ethical approval
Approved by the Institutional Ethics Committee at Seth GS medical college and KEM hospital, Mumbai. Number EC/ CR-07/2023, dated 12/12/2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Sonographic appearance of canal of Nuck hydrocele. Pediatr Radiol. 2007;37:603-6.
- [CrossRef] [PubMed] [Google Scholar]
- Inguinal hernias and hydroceles in infancy and childhood: A consensus statement of the Canadian Association of Paediatric Surgeons. Paediatr Child Health. 2000;5:461-2.
- [CrossRef] [PubMed] [Google Scholar]
- A rare content in inguinal hernial sac, masquerading as scrotal tumour. J Clin Diagn Res. 2013;7:2988-9.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual findings in inguinal hernia surgery: Report of 6 rare cases. Hippokratia. 2009;13:169-71.
- [Google Scholar]
- Inguinal hernia containing uterus and uterine adnexa in female infants: Report of two cases. Pediatr Neonatol. 2011;52:103-5.
- [CrossRef] [PubMed] [Google Scholar]
- Adult intussusception in hernial sac: A case report. J Clin Med Res. 2009;1:119-20.
- [CrossRef] [PubMed] [Google Scholar]
- Paraduodenal hernia complicated with intussusception: Case report. BMC Surg. 2018;18:120.
- [CrossRef] [PubMed] [Google Scholar]
- Concurrent internal hernia and intussusception after Roux-en-Y gastric bypass. BMJ Case Rep. 2018;2018:bcr2018226617.
- [CrossRef] [PubMed] [Google Scholar]
- Case of umbilical hernia, without a sac or other covering, complicated by intussusception and perforation of the bowel. Ind Med Gaz. 1897;32:460.
- [Google Scholar]
- Risk factors associated with intestinal necrosis in children with failed non-surgical reduction for intussusception. Pediatr Surg Int. 2017;33:575-80.
- [CrossRef] [PubMed] [Google Scholar]
- Patent processus vaginalis: A window to the abdomen. Afr J Paediatr Surg. 2009;6:116-7.
- [CrossRef] [PubMed] [Google Scholar]
- Simple maneuvers to reduce the incidence of false-negative findings for contralateral patent processus vaginalis during laparoscopic hernia repair in children: A comparative study between 2 cohorts. J Pediatr Surg. 2013;48:826-9.
- [CrossRef] [PubMed] [Google Scholar]




