

Translate this page into:
Retroperitoneal homunculus lesion in a newborn male
*Corresponding author: Venkatesh Kasi Arunachalam, Department of Radio-diagnosis, Kovai Medical Center and Hospitals, Coimbatore, Tamil Nadu, India. radvenki79@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rajesh SP, Arunachalam VK, Gunasekaran K, Nagarajan K. Retroperitoneal homunculus lesion in a newborn male. Case Rep Clin Radiol. 2025;3:43-5. doi: 10.25259/CRCR_115_2023
Abstract
Fetiform teratoma is a rare form of teratoma that resembles a malformed fetus due to highly organized differentiation. Most commonly seen arising from ovaries; however, we present a case of fetiform teratoma in the retroperitoneum in a male fetus. It is a unique case, as age, gender, and location point toward fetus-in-fetu where malignant transformation is highly unlikely. Distinction from fetus-in-fetu is necessitated due to malignant transformation in case of the presence of immature elements within.
Keywords
Fetiform teratoma
Fetus in fetu
Homunculus

INTRODUCTION
Fetiform teratomas, also referred to as homunculus, are highly differentiated teratomas resembling a fetus and are uncommonly encountered in the ovaries of women of reproductive age.
CASE REPORT
A 1-month-old male baby presented with abdominal distension with an ultrasound report from another hospital showing a mass lesion in the abdomen. The baby was evaluated with a contrast-enhanced computed tomography (CT) abdomen. The CT showed a large heterogeneous intra-abdominal mass lesion with both cystic and solid components. The lesion also showed a central fat component and coarse, chunky calcifications. Some areas are ossified and appear as appendicular skeletons [Figure 1]. The solid component enhances post contrast images [Figure 2]. The lesion displaces the bowel loops to the right side of the abdomen and stomach superiorly. Superolaterally, the lesion abuts the inferior surface of the right lobe of the liver. In view of fat components, solid enhancing areas, presence of appendicular skeleton, and absence of axial skeleton-like elements; the possibility of fetiform teratoma was raised. The baby underwent laparotomy with resection of a large retroperitoneal teratoma and was sent for histopathology [Figure 3]. Histopathology from multiple sections of the specimen showed all three germ layers, predominantly of mature glia with choroid plexus type of epithelium. Respiratory mucosa lined tissue, surrounded by smooth muscle with seromucinous glands and cartilage. Gastrointestinal (GI) tract represents the esophagus lined by squamous epithelium, stomach lined by fundic and antral mucosa, and small intestine with villous type of lining epithelium and colonic epithelium with crypts identified and well-developed nerve plexus. Multiple tubular bones with evidence of endochondral ossification with hematopoiesis were noted. No immature neuroepithelial elements identified which are essential to make a diagnosis of immature teratoma. Pathologists concluded it as fetiform teratoma as there was no discernible spinal column present, despite the presence of well-differentiated GI and respiratory organs as well as bone tissue. Unfortunately, no genetic analyses to determine zygosity were done on this specimen, which could have solved the dilemma in this unique presentation.
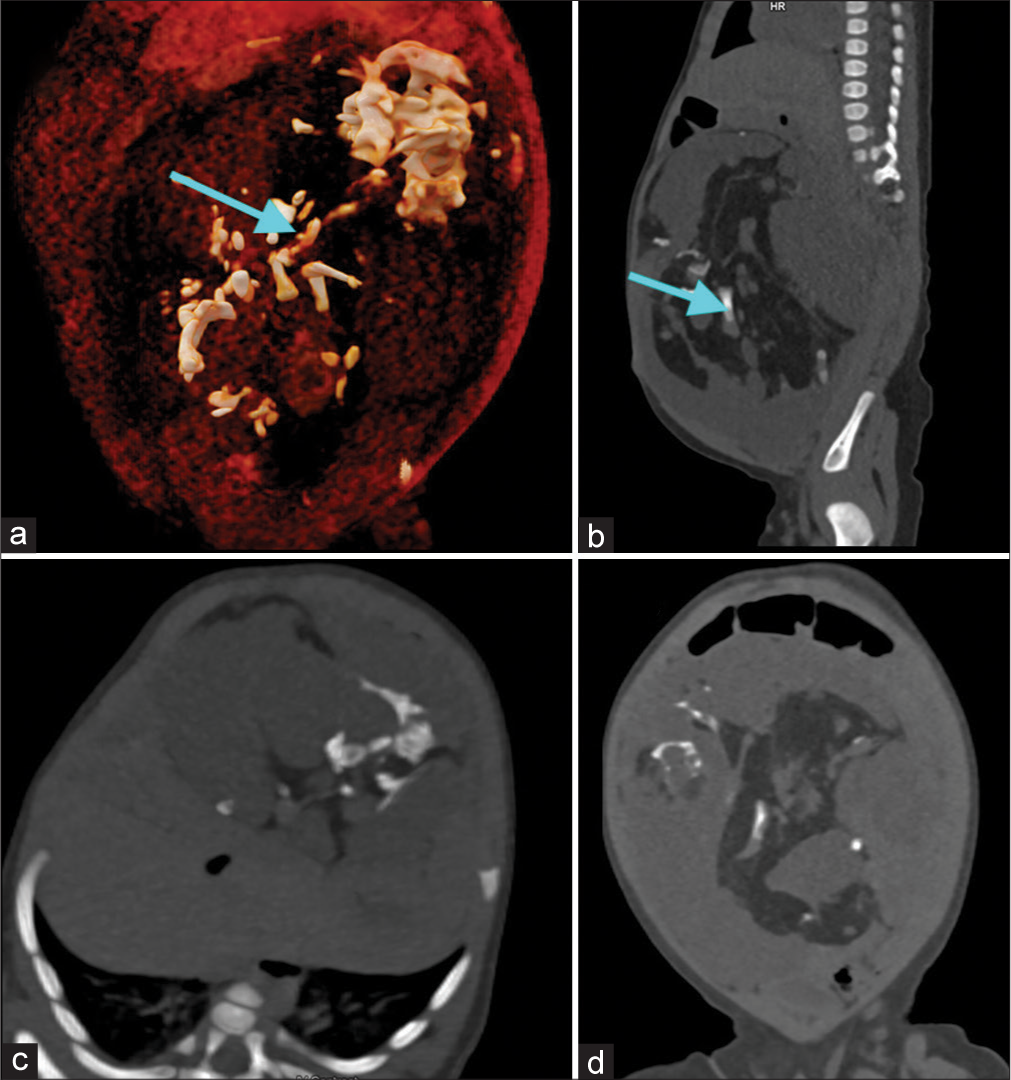
- Plain computed tomography scan images of abdomen; (a) Volume rendered technique image shows appendicular skeleton like elements (blue arrow), (b) oblique sagittal shows appendicular skeleton like elements (blue arrow), (c) oblique axial and (d) oblique coronal images of the abdomen.
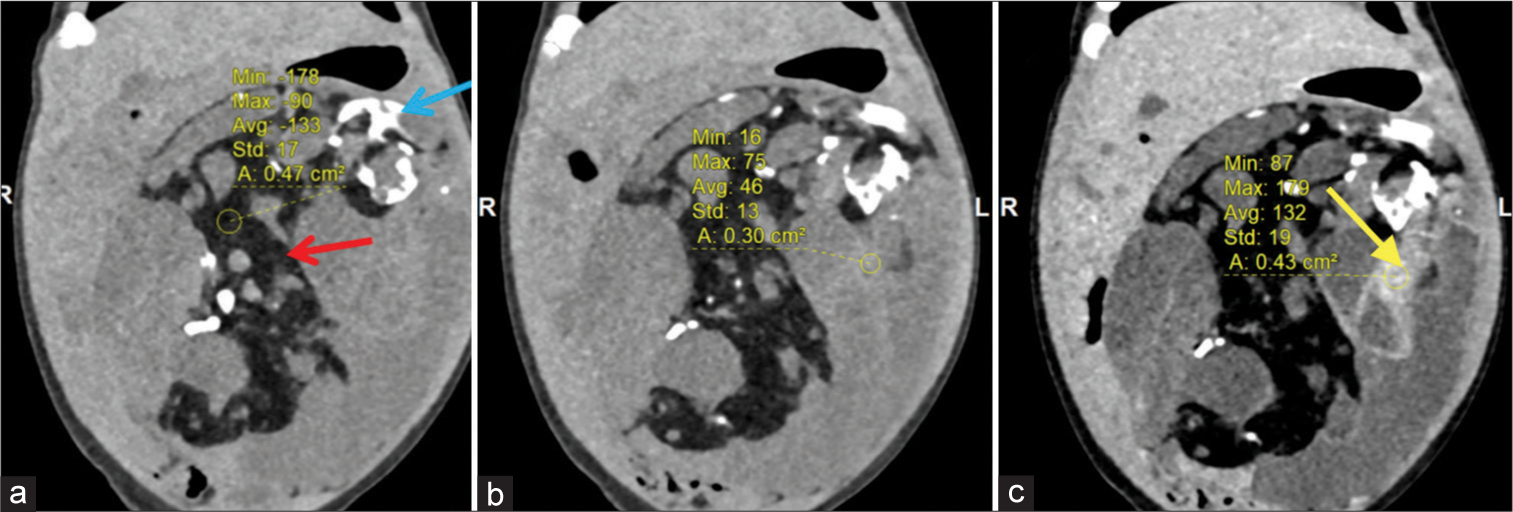
- (a and b) Computed tomography images in coronal plane shows (red arrow) fat components, (blue arrow) coarse chunky calcifications in plain images and (c) venous phase images shows solid enhancing areas (yellow arrow).
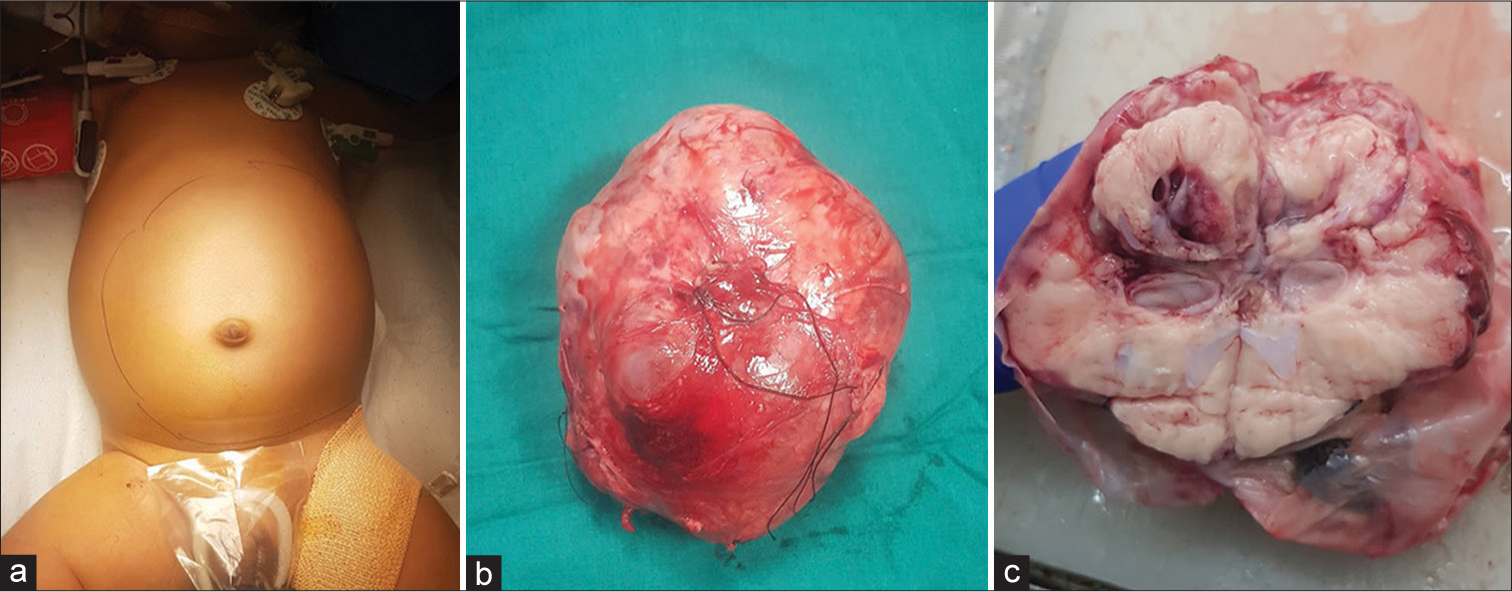
- Clinical picture of the distended abdomen (a) tumor in toto (b) and (c) cuts section of the tumor.
DISCUSSION
Teratoma is a neoplasm that contains two or more germ cell layers. This neoplasm can affect individuals at any age and at any location. Therefore, they can have varying presentations. Among the teratoma, sacrococcygeal teratoma is the most common type in neonatal and infancy periods. Teratomas are mainly categorized into two types; mature and immature. Rarely, mature teratoma shows a high degree of differentiation and may resemble a malformed fetus. This type of teratoma is known as fetiform teratoma. Fetiform teratoma is also known as a homunculus. This is distinguished by the presence of a highly differentiated mass that closely resembles a fetus-like organization. Fetiform teratoma most commonly occurs in ovaries. The other uncommon locations include the cecum, retroperitoneum, and sacrococcyx.[1] The most commonly accepted hypothesis is misplaced blastomere and germ cell development.[2] The closest differential diagnosis for this lesion is the fetus-in-fetu. This is a parasitic monozygotic twin, usually found inside the body of a newborn or infant. Fetus-in-fetu occurs one in 500,000 births and they are diagnosed before the age of 18 months. It occurs most commonly in the retroperitoneum. A few features are used to differentiate fetiform teratoma from fetus-in-fetu. Fetiform teratoma typically develops in ovaries in the reproductive age group, whereas fetus-in-fetu is most frequently localized retroperitoneally in infants. Fetus-in-fetu is most commonly noted in males while fetiform teratoma is more commonly noted in females. On imaging, a vertebral column with internal organs is usually seen in the fetus-in-fetu, but not in fetiform teratomas.[3] Both can also be differentiated based on zygosity. At loci where the normal host tissue exhibits heterozygosity, the majority of ovarian teratomas are homozygous. However, the fetus-in-fetu is always genetically identical to their host. Fetus-in-fetus is often benign; however, fetiform teratoma can develop into a malignant tumor. The subsequent crucial differential diagnosis is ectopic pregnancy. Two essential parameters that differentiate fetiform teratoma from ectopic pregnancy are normal blood beta-human chorionic gonadotropin (HCG) levels and the absence of chorionic villus in histopathologic examination.[4] Fetiform teratoma has a favorable prognosis. Unfortunately, though in most cases, they are benign, 2% of mature cystic teratomas are malignant. In addition, 10% of the lesions may recur following resection.[5] Therefore, total tumor excision is indicated, followed by constant surveillance.
DIFFERENTIAL DIAGNOSIS
Fetus-in-fetu
Lipoblastoma.
CONCLUSION
Fetiform teratoma is a rare form of highly differentiated teratoma resembling a malformed fetus. During the evaluation of fetiform teratoma; the presence of immature neuroepithelial elements needs to be addressed due to its malignant potential. It also needs to be differentiated from fetus-in-fetu and life-threatening conditions like ectopic pregnancy if it is female of reproductive age. Age, gender and beta-HCG correlation need to be done to clinch the diagnosis.
TEACHING POINTS
A young female in the reproductive age group, well-differentiated elements resembling homunculus, arising from ovaries, and fetiform teratoma should be ruled out.
A male infant with a well-differentiated retroperitoneal mass resembling a malformed fetus with internal organs, vertebral body-like structures, fetus-in-fetu should be ruled out.
Close differentials of ectopic pregnancy to be ruled out by beta-HCG levels and chorionic villus in HPE.
MCQs
-
Teratoma with vertebral body-like elements in retroperitoneum?
Fetiform teratoma
Fetus-in-fetu
Ectopic pregnancy
Neuroblastoma
Answer Key: b
-
Post-operative tissue analysis exhibits heterozygosity of mass lesion from host tissue, diagnosis is?
Ectopic pregnancy
Fetus-in-fetu
Fetiform teratoma
Neuroblastoma
Answer Key: c
-
Histopathological analysis of mass lesions from the ovary revealed chorionic villus within with elevated beta-HCG levels; what is the most likely diagnosis?
Ectopic pregnancy
Fetus-in-fetu
Fetiform teratoma
Ectopic pregnancy
Answer Key: d
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Ovarian fetiform teratoma in a 17-year-old adolescent girl. Cureus. 2021;13:e15644.
- [CrossRef] [PubMed] [Google Scholar]
- A rare form of dermoid cyst: A fetiform teratoma. Obstet Gynecol Cases Rev. 2020;7:157.
- [CrossRef] [Google Scholar]
- Fetus in fetu or fetiform teratoma? Report of two cases. J Pediatr Surg Case Rep. 2020;61:101605.
- [CrossRef] [Google Scholar]
- The recurrence rate of ovarian dermoid cysts in pediatric and adolescent girls. J Pediatr Adolesc Gynecol. 2014;27:222-6.
- [CrossRef] [PubMed] [Google Scholar]




