

Translate this page into:
Kartagener syndrome with rare constellation of situs inversus, mesocardia, and congenitally corrected transposition of great arteries

*Corresponding author: Sanjeev Kumar, Department of Cardiovascular Radiology and Endovascular Interventions, All India Institute of Medical Sciences, New Delhi, India. sanjeevradio@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh D, Mukherjee A, Kumar S, Kadiyani L. Kartagener syndrome with rare constellation of situs inversus, mesocardia, and congenitally corrected transposition of great arteries. Case Rep Clin Radiol. doi: 10.25259/CRCR_127_2024
Abstract
Kartagener syndrome (KS) is a rare autosomal recessive condition with a triad of situs inversus, bronchiectasis, and sinusitis. In majority of cases, the heart is structurally normal; however, rarely intracardiac anomalies can be seen in patients with KS such atrial or ventricular septal defects and pulmonary stenosis. We present a rare coexistence of situs inversus, mesocardia, and corrected transposition of great arteries in a young adolescent male with KS diagnosed on computed tomography angiography.
Keywords
Cardiac anomalies
Computed tomography angiography
Kartagener syndrome

INTRODUCTION
Kartagener syndrome (KS) was first described in 1933 by Manes Kartagener as a triad of bronchiectasis, sinusitis, and situs inversus. Clinically patients present with predominant symptoms related to primary ciliary dyskinesia (PCD) ranging from recurrent sinusitis, respiratory tract infections and infertility. Cardiovascular anomalies described in KS are atrial or ventricular septal defects and pulmonary stenosis. We describe a rare coexistence of situs inversus, mesocardia and corrected transposition of great arteries in a young adolescent male with KS diagnosed on computed tomography angiography.
CASE REPORT
A 17-year-old adolescent male visited the cardiology outpatient clinic due to exertional dyspnea for 1 year. The patient also complained of recurrent episodes of sinusitis and chronic cough. Clinical evaluation and rest electrocardiogram (ECG) were unremarkable. Chest radiograph revealed mesocardia with enlarged central pulmonary arteries [Figure 1]. In addition, few cystic radiolucencies were seen clustered in left lower zone accompanied with blunting of left cardio phrenic angle. Further, transthoracic echocardiography revealed atrioventricular and ventriculoarterial discordance suggesting transposition of great arteries. No other associated intracardiac anomalies were detected. Subsequently, the patient underwent a prospective ECG-gated computed tomography angiography (CTA) to evaluate intracardiac and cardiovascular anatomy with simultaneous evaluation of lung parenchyma. Images were reconstructed at 43% (best systole) of the cardiac cycle. CTA revealed heterotaxy phenotype with left bronchial isomerism and visceroatrial situs inversus. Left-sided superior vena cava was seen draining into left-sided morphological right atrium. Pulmonary veins were seen draining into right-sided morphological left atrium. Discordant atrioventricular and ventriculoarterial connections were seen with aorta arising from the right ventricle and pulmonary artery arising from left ventricle. The main, right, and left pulmonary arteries were dilated. Aortic arch was left sided. No other associated anomalies were noted [Figure 2]. The lung window images showed clusters of cystic bronchiectasis in lingula and left lower lobe with air-fluid levels [Figure 3]. A final diagnosis of situs inversus, bronchiectasis, and heterotaxy syndrome with congenitally corrected transposition of great arteries was given. Considering the clinical features and imaging findings, Kartagener syndrome (KS) was the final diagnosis given.
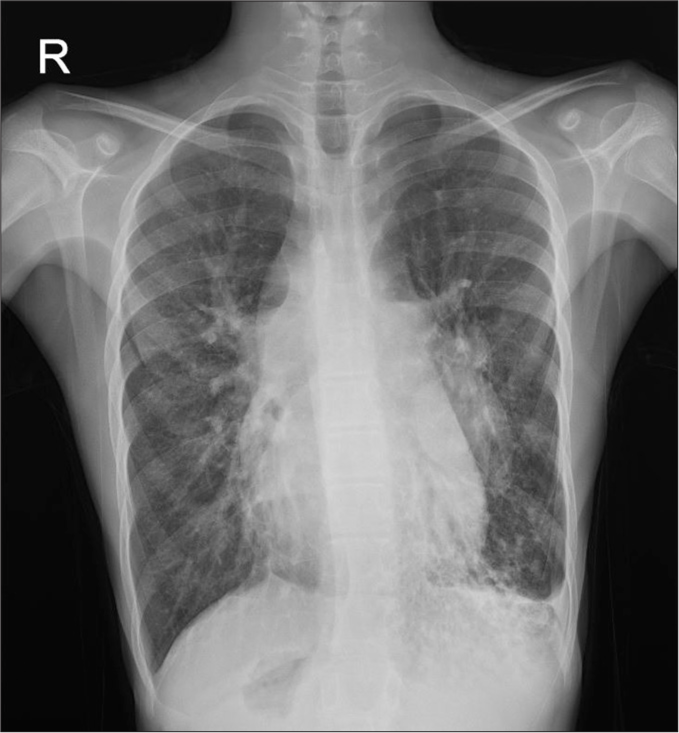
- Chest radiograph showing mesocardia with enlarged central pulmonary arteries. In addition, cystic radiolucencies seen clustered in left lower zone accompanied with blunting of left cardiophrenic angle. R: Right.
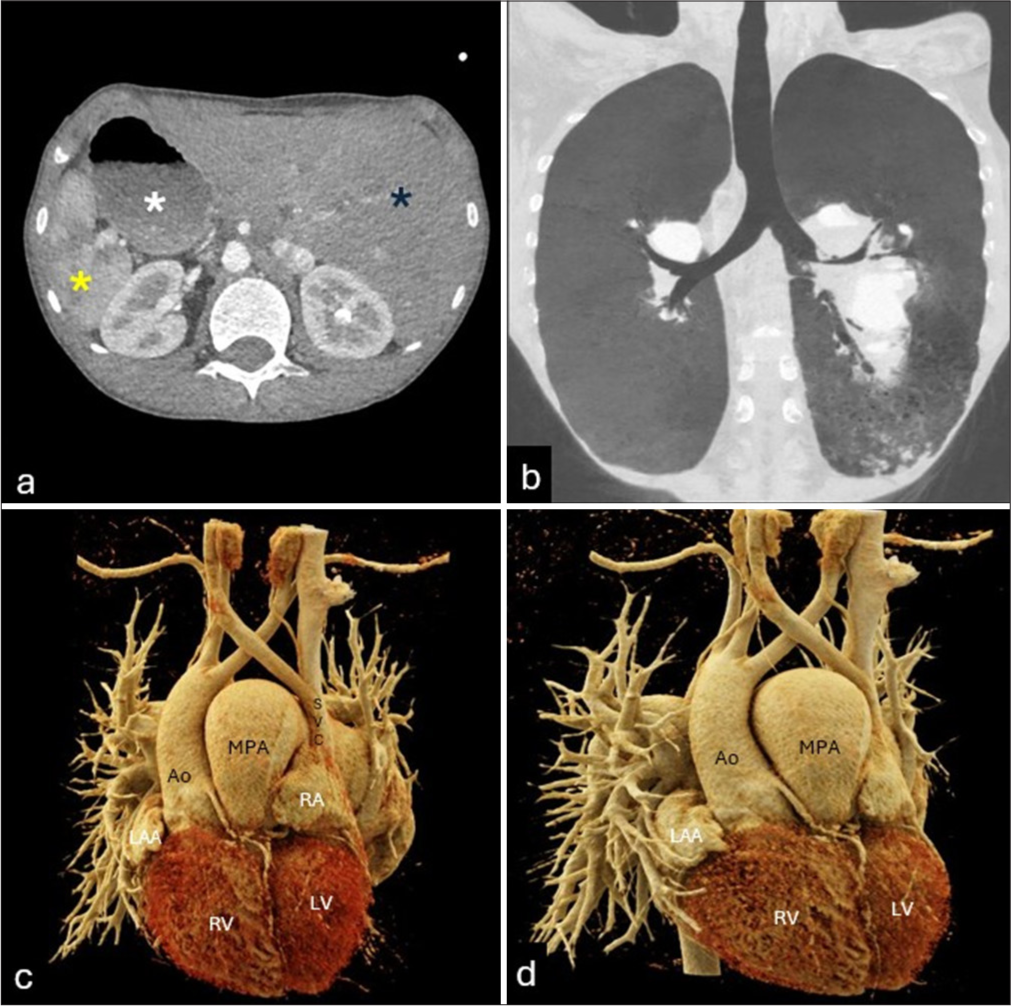
- Computed tomography images (a) showing situs inversus (dark blue asterisk – left-sided liver, yellow asterisk – right-sided spleen, and white asterisk – right-sided stomach). (b) Left isomerism was noted. (c and d) 3D Reconstructed volume rendered images showing atrial situs inversus, left-sided superior SVC connecting to left-sided right atrium. Discordant atrioventricular and ventriculoarterial connections with aorta arising from right ventricle and pulmonary artery arising from left ventricle. Confluent dilated pulmonary arteries seen. Ao: Aorta, LAA: Left atrial appendage, LV: Left ventricle, RA: Right atrium, RV: Right ventricle, SVC: Superior vena cava, MPA: Main pulmonary artery.
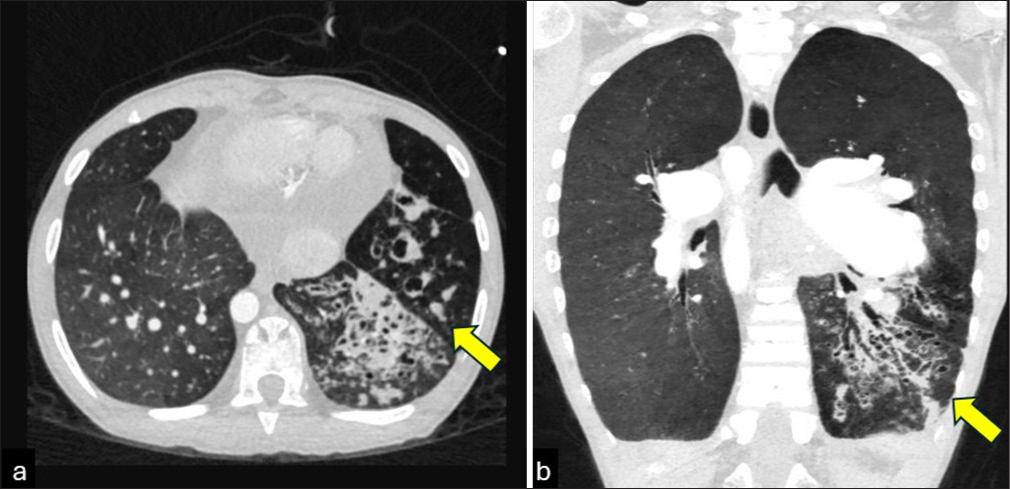
- Computed tomography images in (a and b) axial and coronal plane in lung window showing clusters of cystic bronchiectasis in lingula and left lower lobe with air-fluid levels (yellow arrows).
DISCUSSION
KS was first described in 1933 by Kartagener as a triad of bronchiectasis, sinusitis, and situs inversus. It is a genetic disorder inherited in autosomal recessive pattern.[1] Clinically patients present with predominant symptoms related to primary ciliary dyskinesia ranging from recurrent sinusitis, respiratory tract infections, and infertility. Proposed genetic mutations in Axonemal dynein intermediate-chain gene DNAI1 and DNAH5 genes lead to impaired ciliary motility and disorders of laterality such as heterotaxy syndromes. In general, these patients have a structurally normal heart. Whereas, in conjunction with heterotaxy a higher incidence of cardiovascular anomalies is noted.[2] When present, intracardiac anomalies described in patients with KS are atrial or ventricular septal defects and pulmonary stenosis. Very rarely in KS, discordant atrioventricular and ventriculoarterial connections are described with only three isolated case reports in literature.[3-5] In all the previously described case reports, patients had associated atrial septal defect, ventricular septal defect, or pulmonary stenosis; however, in our index case, no such intracardiac anomaly was detected. The patient was kept on medical management and echocardiography follow-up.
This rare case highlights the sensitivity of CTA in accurately defining intricate thoracic and cardiovascular anatomy as well as pathologies in patients suspected of having KS which potentially directs the further clinical management of such patients.
DIFFERENTIAL DIAGNOSIS
Bronchiectasis, Infective lung changes.
CONCLUSION
CTA is pivotal in defining intricate thoracic and cardiovascular anatomy as well as pathologies in patients suspected of having KS which potentially directs the further clinical management of such patients.
TEACHING POINTS
KS is a rare autosomal recessive condition with a triad of situs inversus, bronchiectasis, and sinusitis. In majority of cases, the heart is structurally normal, however, rarely intracardiac anomalies can be seen in patients with KS such as atrial or ventricular septal defects and pulmonary stenosis.
Proposed genetic mutations in DNAI1 and DNAH5 genes lead to impaired ciliary motility and disorders of laterality such as heterotaxy syndromes.
MCQs
-
Identity the triad seen in KS?
Situs solitus, bronchiectasis, sinusitis
Bronchiectasis, sinusitis, and situs inversus
Bronchiectasis, sinusitis, and dextrocardia
Infertility, sinusitis, recurrent infections
Answer Key: b
-
Mark the correct inheritance pattern of KS?
Autosomal recessive
X-linked recessive
Mitochondrial inheritance
Autosomal dominant
Answer Key: a
-
In corrected transposition of great arteries, identify the correct pair of cardiac connections?
Concordant atrioventricular and ventriculoarterial connections
Discordant atrioventricular and concordant ventriculoarterial connections
Concordant atrioventricular and discordant ventriculoarterial connections
Discordant atrioventricular and ventriculoarterial connections
Answer Key: d
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Zur pathogenese der bronchiektasien bei situs viscerum inversus. Beitr Klin Tuberk. 1933;83:489-501.
- [CrossRef] [Google Scholar]
- Congenital heart disease and other heterotaxic defects in a large cohort of patients with primary Ciliary dyskinesia. Circulation. 2007;115:2814-21.
- [CrossRef] [PubMed] [Google Scholar]
- Dextrocardia and corrected transposition of the great arteries (I,D,D) in a case of Kartagener's syndrome: A unique association. Clin Cardiol. 1998;21:298-9.
- [CrossRef] [PubMed] [Google Scholar]
- Kartagener's syndrome with dextrocardia and corrected transposition of great arteries. Int J Cardiol. 2000;75:305-8.
- [CrossRef] [PubMed] [Google Scholar]
- Kartageners syndrome with corrected transposition: Conducting system studies and coronary arterial occlusion complicating valvular replacement. Chest. 1976;69:677-80.
- [CrossRef] [PubMed] [Google Scholar]




