

Translate this page into:
Diagnostic dilemma – Ovarian dermoid cysts presenting with uncommon complications and a rare association

*Corresponding author: Annapurna Srirambhatla, Department of Radiodiagnosis, All India Institute of Medical Sciences, Bibinagar, Telangana, India. purnasrirambhat@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Patle A, Kapoor M, Srirambhatla A, Arora AJ. Diagnostic dilemma – Ovarian dermoid cysts presenting with uncommon complications and a rare association. Case Rep Clin Radiol. doi: 10.25259/CRCR_192_2023
Abstract
Mature cystic teratomas, also known as dermoid cysts, are commonly encountered ovarian tumors accounting for up to 10–25% of all ovarian neoplasms. Mostly asymptomatic and incidentally detected, they may present with associated complications such as torsion, rupture, malignant transformation, and infection. Fistulization of ovarian cysts into the bowel is a rare complication and occurs in cases of infection or malignant transformation. We present a rare case of an infected dermoid cyst with co-existing endometriosis and fistulization into the rectum in a 35-year-old female. The patient presented with fever, pain, and history of infertility. This article highlights the important differential diagnosis to be considered in a multiloculated ovarian cyst containing fat and pockets of air.
Keywords
Dermoid cyst
Enteric fistula
Endometriosis
Ovarian tumor
Infertility

INTRODUCTION
Dermoid cysts are commonly encountered fat-containing ovarian tumors accounting for 10– 20% of all ovarian neoplasms.[1] The presence of sebaceous/fat components and calcifications makes the diagnosis of most dermoid cysts easy. They are usually asymptomatic and incidentally detected but may occasionally present with associated complications. We present a case of an infected dermoid cyst with co-existent endometriosis showing fistulous communication with the rectum and discuss the important differential diagnosis to be considered in a multiloculated ovarian cyst containing fat and pockets of air. This case is rare because enteric fistulization is an uncommon complication of dermoid cysts and to our knowledge, very few cases of dermoid cysts associated with endometriosis have been reported in literature.
CASE REPORT
A 35-year-old nulliparous female presented with complaints of diffuse pain abdomen for 1 month, fever with chills, and burning micturition for 1 week. The patient gave a history of primary infertility with amenorrhea for 1 year. On examination, abdominal distention was present with mild tenderness in the left iliac fossa. Per vaginal examination revealed a palpable large cystic mass predominantly in the left adnexa and in the Pouch of Douglas (POD). Blood investigations revealed leukocytosis and the urine examination was insignificant.
Imaging findings
Transabdominal ultrasound revealed a large thick-walled, multiloculated, cystic lesion arising from the pelvis (bilateral adnexa) extending into the lower abdomen with a few of the locules showing echogenic “dots and dashes” pattern [Figure 1a and b]. A curvilinear hyperechoic lesion with shadowing suggestive of fat was seen in the non-dependent portions [Figure 1c]. Few of the locules showed echogenic foci with reverberation artifacts suggestive of air [Figure 1d]. Grade 2 vascularity was noted in the wall of the lesion. There were no solid components/mural nodules. Normal ovarian parenchyma could not be separately visualized. The uterus was straddled between the lesions. Minimal ascites was noted. Few small volume para-aortic nodes were seen. A diagnosis of ovarian dermoid with likely infection was made.

- Ultrasound images of lower abdomen and pelvis, transverse view. (a) Multiloculated cystic lesion (white asterisk) showing linear echogenic lines (white arrow). (b) Cyst shows thick walls (white asterisk) and echogenic contents (white arrow), (c) Intra cystic calcification with shadowing (white long arrow) and ‘dots and dashes’ appearance (white short arrow), (d) Reverberation artefacts from air within the cyst (white arrow).
Contrast-enhanced computed tomography (CECT) of the abdomen revealed a thick-walled multiloculated cystic lesion arising from bilateral adnexa extending into the lower abdomen and POD measuring 10 × 9 × 11 cm. Smooth homogenous enhancement of the cyst wall and septations was noted [Figure 2a and b]. Few of the locules showed small specks of air and fat [Figure 2a-d]. No solid components or mural nodules were seen. The cyst was closely abutting the rectum. Minimally enhancing paraaortic nodes measuring 12 mm in the short axis were noted. Minimal ascites was seen. With these findings, differential diagnosis included (1) dermoid cyst with likely infection adherent to the rectum and (2) cystic ovarian neoplasm (intermediate concern) with co-existing dermoid and fistulization into the bowel.
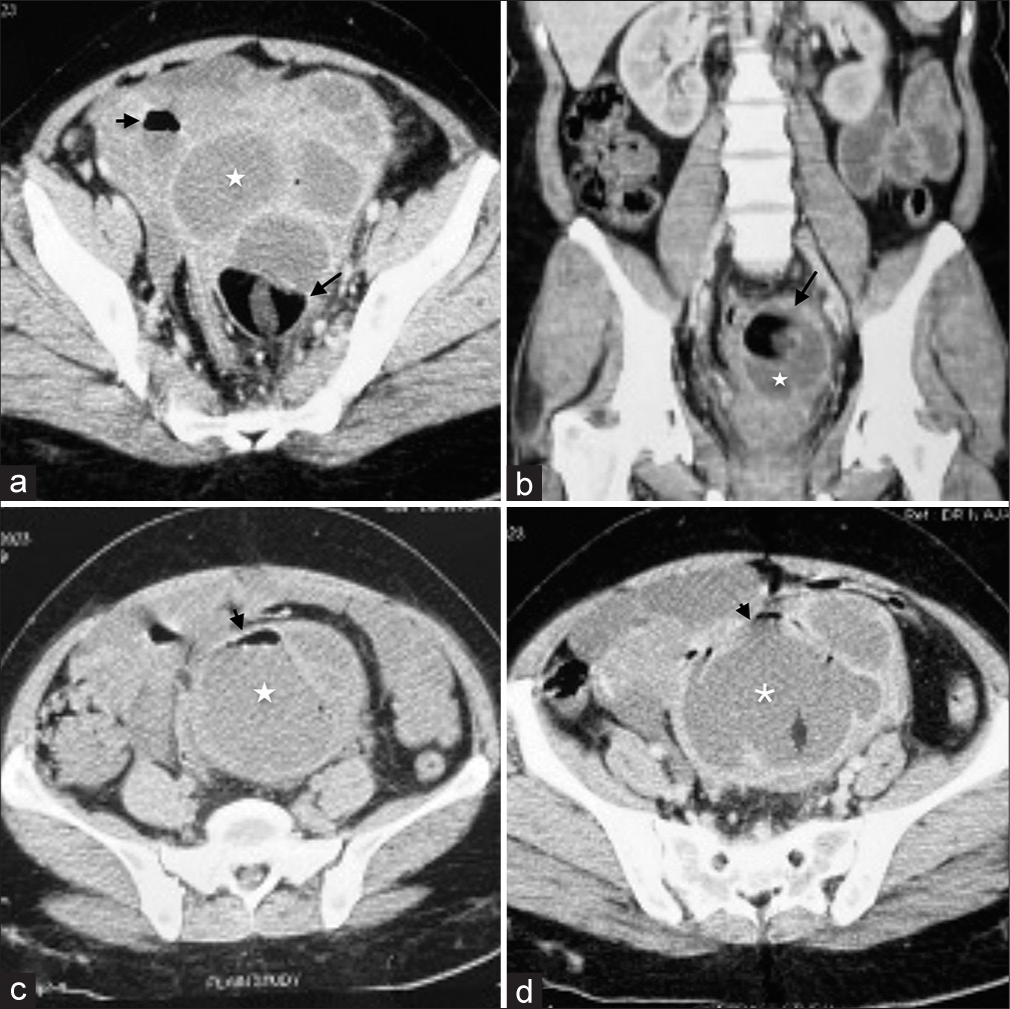
- CT images of the pelvic mass. (a) Axial CECT image shows multiloculated cystic lesion (white asterisk) with enhancing walls and septations, fatty components (black long arrow) and small pocket of air (black short arrow), (b) Coronal CECT image shows the fatty component (white asterisk) and wall enhancement (black arrow), (c) Non contrast axial image shows air-fluid level (black arrow) in the cyst (white asterisk), (d) Axial post contrast image showing multiloculated cyst with enhancing walls and septations (white asterisk) and air pockets (black arrow).
Treatment
The patient underwent bilateral salpingo-oophorectomy, total abdominal hysterectomy, infra colic omentectomy, and primary repair of the rectum. Intraoperative findings were of bilateral multiloculated cystic lesions with pus and hair (dermoid cysts) showing dense adhesions with the anterior rectal wall. Fistulous communication of the rectum with the cyst was seen 20 cm proximal to the anal verge. Dilatation of the proximal small bowel loops was noted with approximately 100 mL of ascites.
Histopathology
Gross specimen showed enlarged ovaries with bosselated appearance with fat, hair, and hemorrhagic pultaceous material [Figure 3a]. Histopathology examination was suggestive of mature cystic teratoma [Figure 3b] involving both ovaries with granulo-suppurative inflammation [Figure 3c]. Small areas of endometriosis [Figure 3d] were seen in the left ovary. Stains for tuberculosis bacteria and fungi were negative.
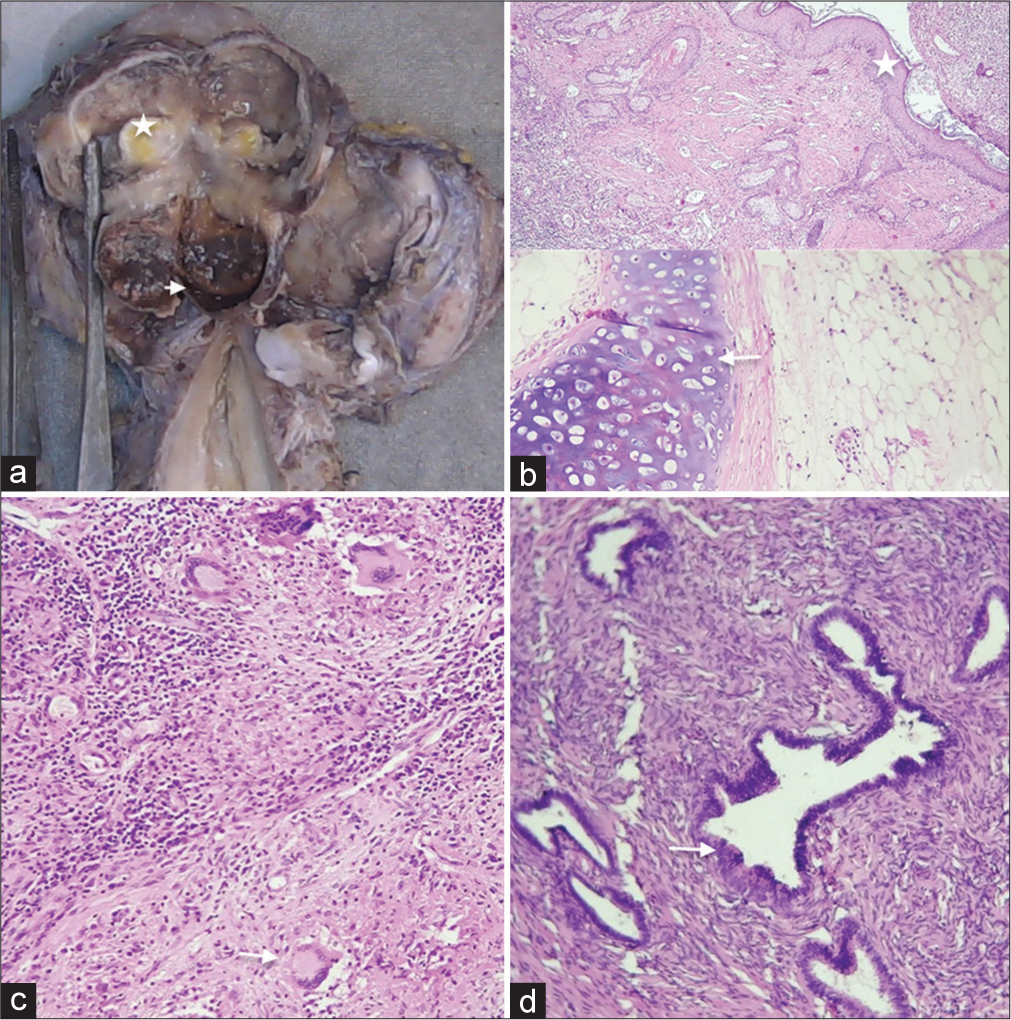
- Gross and histopathology. (a) Gross specimen of the ovaries showing the fatty (white asterisk) and the endometriotic (white arrowhead) components which are seen as “chocolate”/hemorrhagic components in the enlarged ovary. (b) Ovarian cyst lined by squamous epithelium (white asterisk) containing adipose and mature cartilage (white arrow) components suggestive of dermoid. (c) Areas of granulosuppurative inflammation with Langerhans-type giant cells (white arrow). (d) Endometriotic glands (white arrow) with hemorrhage in the ovaries.
DISCUSSION
The complications associated with dermoid cysts are torsion (16%), infection (1%), rupture (1–4%), malignant transformation (1–2%), or autoimmune hemolytic anemia.[2] Differential diagnosis for abdominal pain in women with ovarian cysts may include tubo-ovarian abscess, torsion, or infection. Infection of dermoid cysts is relatively rare and is usually due to coliform bacteria.[2,3] Patients present with abdominal pain, fever, vomiting, and leukocytosis (as in our case). In such a scenario, it is important to rule out torsion, which is a more common complication.
The presence of granulomatous tissue on histology raised the suspicion of tubercular infection in our case; however, mycobacteria could not be isolated and the stains were negative. Tubercular infection of the ovaries occurs in 20– 30% of women with genital tuberculosis. It is mostly bilateral and results in adhesions resulting in the formation of tuboovarian masses/abscesses.[4] Peritoneal spread with omental thickening, enlarged nodes, and ascites can occur.
Fistulization of dermoid cysts into adjacent viscera is a very rare complication, the common sites being into the urinary bladder, rectum, small bowel, sigmoid colon, and vagina. Fistula formation has been postulated to result from weakening of the cyst wall by repeated vascular insults secondary to torsion-detorsion, infection, adhesions or rarely malignant transformation.[3,5]
Malignant transformation occurs more commonly in the older age group. Imaging findings of such a transformation are enhancing solid components and/or transmural extension of the Rokitansky nodule.[3,6] Due to the paucity of fat components, a differential of a collision tumor was considered. Collision tumors are two histologically distinct tumors present adjacent to each other with no admixture of tissues. The most common collision tumors to occur with dermoid cysts are mucinous cystadenoma/cystadenocarcinoma.[2] More of a histological diagnosis, collision tumors show the presence of two separate cystic lesions on imaging, one of which is dermoid.
The co-existence of dermoid cysts and endometriosis in the same ovary is very rare with very few cases reported in literature.[7] Most of the cases reported were in young women. The common presentation was abdominal pain or infertility. Of note was that the diagnosis of co-existing pathologies was made through magnetic resonance imaging (MRI) followed by confirmation of histopathology.[7] The importance of this association was atypical imaging features on ultrasound which may raise the suspicion of malignancy.
CONCLUSION
Infection and/or fistulization are two uncommon complications to be considered in dermoid cysts showing air pockets. Dermoid cysts with associated endometriosis are a rarer occurrence, diagnosed mainly on MRI and confirmed by histopathology.
MCQs
-
The most common complication of ovarian dermoid cysts is:
Infection
Torsion
Rupture
Malignancy
Answer Key: b
-
The features suggestive of malignant transformation in a dermoid cyst are:
Enhancing solid components
Transmural extension of Rokitansky nodule
Presence of ascites
Both a and b
Answer Key: d
-
What is a collision tumor?
Presence of two different histopathologies in the same tumor
Infection within the tumor
Presence of two tumors adjacent to one another with no admixture of tissues
Presence of two tumors adjacent to one another with an admixture of tissues
Answer Key: c
Acknowlegment
Dr. Mishu Mangla - Department of Obstetrics and Gynaecology and Dr. Tushaar Parmeshwar - Department of General Surgery, AIIMS Bibinagar, Dr. Mishu Mangla, Department of Obstetrics and Gynaecology, AIIMS Bibinagar, Dr. Tushaar Parmeshwar, Department of General Surgery, AIIMS Bibinagar, Dr. Tara Roshni Paul, Professor, Department of Pathology, Nizam’s Institute of Medical Sciences.
Ethical approval
The Institutional Review Board has exempted from review and given the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- An unusual presentation of ovarian teratoma: A case report. Case Rep Emerg Med. 2012;2012:845198.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging findings of complications and unusual manifestations of ovarian teratomas. Radiographics. 2008;28:969-83.
- [CrossRef] [PubMed] [Google Scholar]
- Atypical CT and MRI manifestations of mature ovarian cystic teratomas. AJR Am J Roentgenol. 2004;183:743-50.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging manifestations of genitourinary tuberculosis. Radiographics. 2021;41:1123-43.
- [CrossRef] [PubMed] [Google Scholar]
- CT depiction of ovarian dermoid showing spontaneous fistulous communication with small bowel. Egypt J Radiol Nucl Med. 2018;49:292-4.
- [CrossRef] [Google Scholar]
- Ovarian teratomas: Tumor types and imaging characteristics. RadioGraphics. 2001;21:475-90.
- [CrossRef] [PubMed] [Google Scholar]
- Endometriosis coexisting with mature cystic teratoma in the same ovary and ectopic pregnancy of left fallopian tube: A rare coexistence. Clin Case Rep. 2015;3:315-8.
- [CrossRef] [PubMed] [Google Scholar]




