

Translate this page into:
Thyroglossal cyst with intralaryngeal extension – An unusual case report

*Corresponding author: Vineet Kumar Vemuri, Department of Radiodiagnosis, GITAM Institute of Medical Sciences and Research, Visakhapatanam, Andhra Pradesh, India. vineetradiology97@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vemuri VK, Mallik GR, Vemuri NV. Thyroglossal cyst with intralaryngeal extension – An unusual case report. Case Rep Clin Radiol. doi: 10.25259/CRCR_99_2024
Abstract
Thyroglossal duct cysts are the most prevalent congenital neck masses originating from thyroglossal duct remnants. Here, we present a case of thyroglossal dust cyst with hoarseness and difficulty breathing. A contrast-enhanced computed tomography scan confirmed the intra-laryngeal extension and airway compromise. Sistrunk procedure along with laryngeal reconstruction was done. Histopathology confirmed thyroid follicles in the cyst wall.
Keywords
Thyroglossal cyst
Air way obstruction
Symptomatic presentation

INTRODUCTION
Thyroglossal duct cysts (TGDCs) are the most common congenital neck masses in children, but they can also present in adults.[1] These account for 70% of all congenital neck anomalies.[2] TGDCs are usually located in the midline of the neck; often presenting as a painless, fluctuant mass that may move with swallowing or protrusion of the tongue.
Laryngeal extension of TGDCs by causing erosion of the thyroid cartilage or thyrohyoid membrane is an uncommon but significant variation that poses unique diagnostic and therapeutic challenges. When these cysts extend into the laryngeal framework, they can cause symptoms such as dysphagia, dysphonia, and airway obstruction which are atypical for more common presentations of TGDCs.
CASE REPORT
A middle-aged man presented with a history of neck swelling over anterior aspect of the neck since 2 months. He complained of progressive hoarseness of voice and difficulty in breathing and swallowing since 1 month. He presented with acute exacerbation of the symptoms since 1 week.
Clinical examination and laryngoscopy was done for complaints of difficulty in breathing and was found to have significant airway obstruction from external compression. He underwent emergency tracheostomy to stabilize the airway and was sent for further imaging.
Radiograph of neck in anteroposterior and lateral views was done before acute presentation which was reviewed. The radiograph showed homogeneous soft-tissue density neck swelling in the lower anterior neck with airway narrowing at the level of hypopharynx and supraglottic larynx [Figure 1].
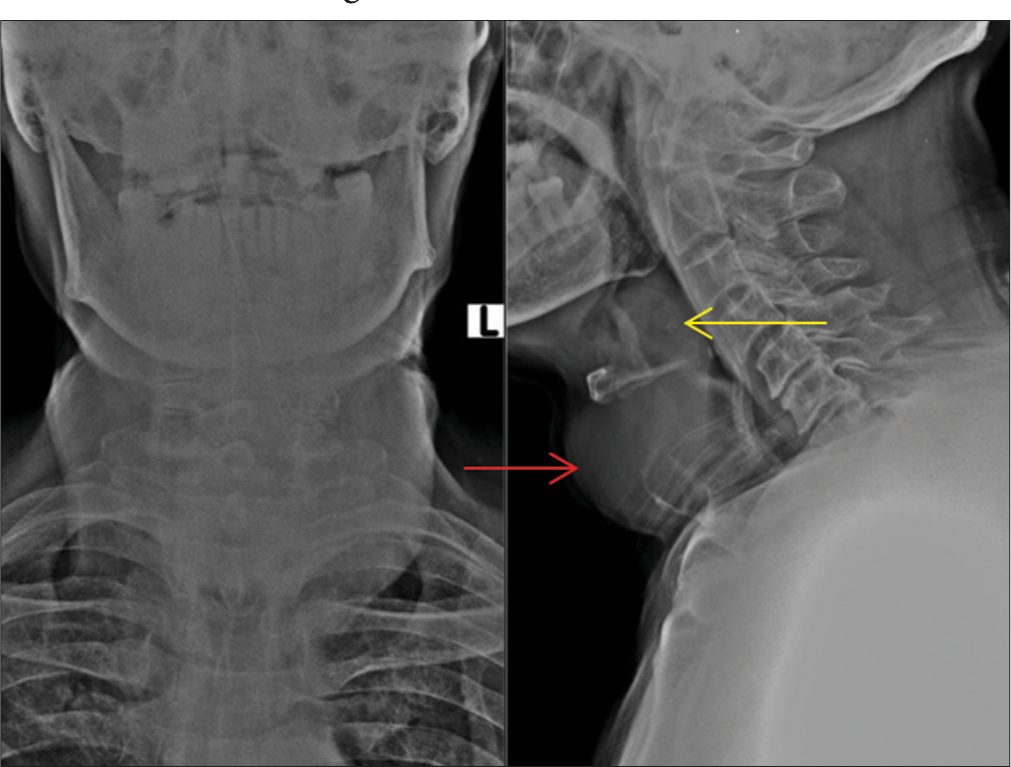
- Anteroposterior and lateral radiograph of neck. Lateral radiograph showing diffuse soft-tissue swelling (red arrow) with airway narrowing at the level of hypopharynx and supraglottic larynx (yellow arrow).
Contrast enhanced computed tomography (CT) scan of neck revealed a well-defined, uniformly thin-walled cystic lesion measuring 4.5 × 3.8 × 2.2 cm in the anterior lower third of the neck extending to left paramedian plane underneath the left sternocleidomastoid muscle spanning from C5 to T1 vertebral levels craniocaudally.
The cyst was extending into the larynx at infrahyoid level compressing the supraglottic air column through a midline defect in the thyrohyoid membrane [Figure 2a]. The intralaryngeal component measured 6.0 × 3.5 × 3.0 cm extended from C2 to C5 level. It was seen pushing the epiglottis to the right side and there was a near total narrowing of the supraglottic air column at the level of the hyoid [Figure 2b and c]. The cranial end of the intra-laryngeal extension was indenting the base of the tongue in pre-epiglottic space [Figure 2d]. Post-contrast minimal enhancement of the cyst wall was present.

- (a) Plain computed tomography (CT) scan of the neck shows a well-defined uniform cystic lesion in the anterior neck underneath the left sternocleidomastoid muscle with a breach in the thyrohyoid membrane at the infrahyoid level and intralaryngeal extension (red arrow). (b) Axial sections of contrast-enhanced CT demonstrated intra-laryngeal extension with compression of the airway column (red arrow). (c) The coronal section of contrast-enhanced CT demonstrated a breach in the thyrohyoid membrane (red arrow) and cranial extension of the cyst into the larynx. The tracheostomy tube (yellow arrow) can be seen in situ with air in the soft-tissue facial planes. (d) The sagittal section of contrast-enhanced CT shows the infrahyoid relation of the thyroglossal cyst with the intra-laryngeal component indenting the base of the tongue (red arrow).
The tracheostomy tube can be identified in situ with air foci within the soft tissue and neck facial planes consistent with surgical emphysema secondary to intubation.
The patient was followed up and sistrunk procedure was done to excise the cyst and laryngeal reconstruction was done [Figure 3]. The excised cyst was sent for histopathological examination. Sections studied showed fibrocollageneous cyst wall focally lined with ciliated columnar epithelium with few thyroid follicles and lymphoid aggregated. There is no evidence of any malignant cells in the studied histopathological sections.

- (a) Pre-operative image of the neck swelling. (b) Intraoperative image shows the excised cyst.
DISCUSSION
The thyroglossal duct atrophies and disappears between the 7th and 10th weeks of gestation.
Persistent remnants of the thyroglossal duct are thought to be the source of TGDC.[3] The disease can be seen in children and adults and there appears to be a bimodal distribution of its presentation (1st and 5th decades).[1] A TGDC typically presents as a midline neck mass, often following an upper respiratory tract infection. Occasionally, a TGDC may also present with hoarseness or dysphagia.[4]
The rare occurrence of TGDCs with laryngeal extension underscores the importance of considering diverse differential diagnoses for neck masses. Imaging techniques like CT are helpful for further imaging, precise location, and treatment planning in such complex cases. The presence of a laryngeal extension with airway obstruction necessitates a thorough evaluation and swift imaging to delineate the extent of the lesion and its relationship to surrounding structures.[5]
This case highlights the significance of taking TGDCs into account when making a differential diagnosis of neck mass including the larynx and addresses the therapeutic and prognostic consequences. Multidisciplinary teamwork involving otolaryngologists, radiologists, and surgeons is crucial for optimal patient management.
DIFFERENTIAL DIAGNOSIS
The differential diagnoses for anterior neck cystic lesions are laryngocele, brachial cleft cyst, and epidermoid cyst [Table 1]. Both laryngocele and TGDCs can extend through thyrohyoid membrane but the TGDC will not involve laryngeal ventricle.[6] Sometimes laryngocele can be air filled or show air fluid levels due to communication with the airway.
| Differential diagnosis | Differentiating feature | |
|---|---|---|
| 1 | Laryngocele | Laryngocele involve laryngeal ventricle and may contain air or air fluid levels as they communicate with the airway |
| 2 | Brachial cleft cyst | Usually away from the midline |
| 3 | Epidermoid cyst | Subcutaneous in location and are found superficial to strap muscles |
CONCLUSION
The significance of taking TGDCs into account while making a differential diagnosis of neck tumors with unusual presentations, such laryngeal involvement, is demonstrated by this instance. Advanced imaging and meticulous surgical planning are crucial for effective management. Our experience underscores the need for heightened awareness and comprehensive evaluation to ensure accurate diagnosis and appropriate treatment of TGDCs with laryngeal extension.
TEACHING POINTS
Close relationship with posterior aspect of hyoid bone is an important differentiating feature of thyroglossal duct cyst.
Hoarseness is relatively rare complaint with thyroglossal cyst, which when present must alert underlying encroachment and destruction of larynx.
MCQ’S
-
Most common location of thyroglossal duct cyst
Suprahyoid
Infrahyoid
Sublingual
Thyroid cartilage
Answer key: b
-
Most common malignancy in thyroglossal duct cyst
Medullary carcinoma
Squamous cell carcinoma
Papillary carcinoma
Follicular carcinoma
Answer key: c
-
Sistrunk procedure involves all of the following except
Thyroidectomy with surrounding tissue
Thyroglossal duct cyst excision
Middle part of hyoid bone
Thyroglossal tract and surrounding tissue
Answer key: a
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Thyroglossal duct cysts: Presentation and management in children versus adults. Int J Pediatr Otorhinolaryngol. 2003;67:1285-90.
- [CrossRef] [PubMed] [Google Scholar]
- Review of head and neck lesions in infancy and childhood. Surg Clin North Am. 1992;72:1429-47.
- [CrossRef] [PubMed] [Google Scholar]
- A Clinicopathologic series of 685 thyroglossal duct remnant cysts. Head Neck Pathol. 2016;10:465-74.
- [CrossRef] [PubMed] [Google Scholar]
- Large thyroglossal duct cyst with laryngeal extension. Head Neck. 1994;16:586-8.
- [CrossRef] [PubMed] [Google Scholar]
- Thyroglossal duct cyst-more than just an embryological remnant. Indian J Surg. 2011;73:28-31.
- [CrossRef] [PubMed] [Google Scholar]
- Cystic masses of neck: A pictorial review. Indian J Radiol Imaging. 2012;22:334-43.
- [CrossRef] [PubMed] [Google Scholar]




