

Translate this page into:
The “expanded Goldenhar syndrome” – A rare entity
*Corresponding author: Neha Nischal, Department of Radiology, Holy Family Hospital, New Delhi, Delhi, India. neha.nischal@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Utkarsh S, Sharma P, Tyagi H, Nischal N. The “expanded Goldenhar syndrome” – A rare entity. Case Rep Clin Radiol. doi: 10.25259/CRCR_6_2024
Abstract
Goldenhar syndrome is a rare congenital condition occurring due to defects in the first and second branchial arches and encompasses a wide range of anomalies involving craniofacial structures, vertebrae, and internal organs, typically manifesting unilaterally. The causes for the defects are heterogenous with most cases being sporadic; however, the exact etiology of the disorder is still unknown. In this case report, we present a case of an adult male presenting with features of Goldenhar syndrome with ipsilateral pulmonary aplasia, which is a rare association.
Keywords
Goldenhar syndrome
Oculoauricular dysplasia
Pulmonary aplasia
Vertebral anomalies

INTRODUCTION
Goldenhar syndrome is a complex malformation of the structures arising from the first and second branchial arches, the first pharyngeal pouch, the first branchial cleft, and the primordia of the temporal bone affecting them to varying degrees.[1]
Goldenhar syndrome was described by a Swiss ophthalmologist, Dr. Maurice Goldenhar in 1952 as oculoauricular dysplasia consisting of preauricular appendages, fistulas, and epibulbar dermoids. Subsequently, Gorlin et al. added vertebral anomalies to the syndrome and the name oculo-auriculo-vertebral (OAV) dysplasia was suggested.[2] The term facio-auriculo-vertebral sequence was used by Smith (1978) to include both Goldenhar syndrome and hemifacial microsomia in the spectrum of this disorder.[3]
Ocular findings include epibulbar dermoids and/or lipodermoids, unilateral coloboma of the upper lid, anophthalmia, microphthalmia, microcornea, coloboma of iris or choroid, and iris atrophy or polar cataract. Auricular findings include preauricular appendages, blind-ended fistulas, deformities of the external ear such as microtia, absence or deficiency of external auditory meatus, and conduction deafness. Oral manifestations include micrognathia and/or unilateral hypoplasia (aplasia) of the mandibular ramus and condyle causing malocclusion of teeth, cleft lip/palate, bifid tongue, bifid uvula, double lingual frenulum, high palatal vault, and mild maxillary hypoplasia. Vertebral anomalies include atlas occipitalization, synostosis, hemivertebrae, fused vertebrae, scoliosis, and bifid spine.[4] Other major organ system anomalies include cardiac structural defects, renal agenesis, pulmonary agenesis, and vascular anomalies.[5]
The association of other organ systems has been coined as the “expanded Goldenhar complex.”[6] There have been only a few reports of pulmonary anomalies associated with Goldenhar syndrome. Lung involvement usually coincides with facial anomalies on the corresponding side.[7-9] The association of contralateral pulmonary involvement with Goldenhar syndrome is extremely rare.[10,11]
CASE REPORT
A 21-year-old boy presented to the plastic surgery department with complaints of facial asymmetry and for the surgical correction of cleft palate. The patient was a product of nonconsanguineous marriage with an uneventful antenatal and birth history. There was no antenatal infection or maternal drug intake history during the pregnancy. The developmental milestones were normal.
On clinical examination, the patient had an asymmetric face with flattening of the left side. The left pinna was low set and malformed with no identifiable structures and nonvisualization of the external auditory meatus. A small preauricular skin tag was present. Examination of the oral cavity revealed an incompletely formed soft palate [Figure 1]. The right pinna was well developed. Eye examination was normal. The rest of the systemic examination was also within normal limits.

- Frontal photograph (a) shows facial asymmetry with flattening of the left side and cleft palate (white arrow). Lateral photograph (b) shows the low set, rudimentary left pinna (black arrow).
Since the patient was a previously known case of pulmonary aplasia computed tomography (CT) scan done in childhood for recurrent chest infections, records were not available, he was referred to the radiology department for an X-ray and CT scan of the thorax as part of the pre-anesthetic evaluation.
Chest radiograph revealed near-complete opacification of the left hemithorax with an ipsilateral shift of the trachea and mediastinum. Vertebral anomalies were noted [Figure 2]. The right lung was overinflated but otherwise unremarkable.

- Frontal chest radiograph (a) reveals opaque left hemithorax with loss of volume and crowding of ribs. There is tracheomediastinal shift and transmediastinal herniation of the right lung toward left side. Anomalies of dorsal vertebrae are also noted with semi-segmented hemivertebra at D8-D9 level (white arrow). Coronal minimum intensity projection reformatted image of contrast-enhanced computed tomography (CECT) chest (b) shows aplastic left lung with the rudimentary, blind ending left main bronchus (black arrow). Axial contrast-enhanced computed tomography scan of thorax (c) reveals continuation of main pulmonary trunk (black star) into the right pulmonary artery (double black arrowhead) with absence of the left pulmonary artery. Coronal reformatted image of CECT thorax in bone window settings (d) shows only right pulmonary veins (white arrows) draining into the left atrium (yellow star) with absence of the left pulmonary veins.
CT scan of the chest revealed complete absence of the left lung parenchyma with evidence of a rudimentary, blind-ending left bronchus, and absence of the left pulmonary artery as well as the left pulmonary veins. There was resultant ipsilateral tracheal and mediastinal shift with rotation of the cardiac axis. The right lung was overinflated but otherwise normal. The main pulmonary artery continued as the right pulmonary artery [Figure 2]. Complex vertebral segmentation-fusion anomalies were noted in the cervicodorsal spine.
High-resolution CT of the temporal bones was also performed, revealing microtia on the left side with the absence of external auditory meatus and canal. The left middle ear cavity was atretic with non-visualization of ossicles. The inner ear structures appear normal. Nonpneumatization of the left mastoid air cells was also noted. The right pinna, external auditory meatus and canal, and the right middle ear cavity and inner ear cavity appeared unremarkable. The left hemimandible was also underdeveloped [Figure 3].
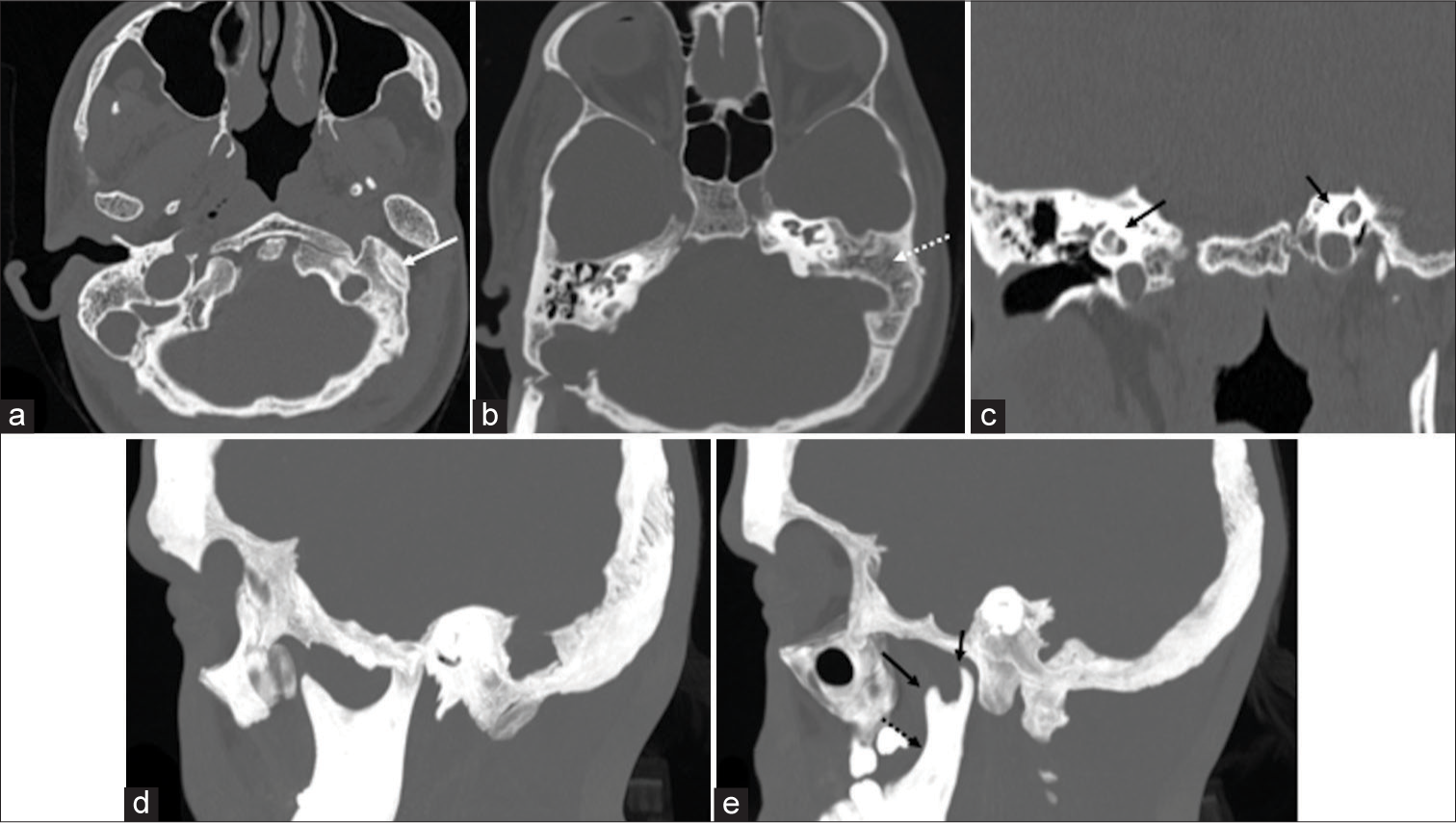
- Axial section (a) of HRCT temporal bones reveals atretic left external and middle ear cavities (white arrow). Axial section at a cranial level (b) shows non-pneumatization of left mastoid air cells (white dashed arrow). Coronal section (c) reveals normal bilateral cochlea (black arrows). Sagittal reformatted HRCT temporal bone images (d and e) in maximum intensity projection show normally developed right mandible (d) and hypoplastic left mandibular ramus (black dashed arrow in e), coronoid and condylar processes (black arrows in e).
DISCUSSION
Goldenhar syndrome, also known as OAV dysplasia, is complex and incompletely understood continuum of disorders of unknown etiology. It is a complex developmental disorder involving eyes, ears, face, spine, etc., which are affected to varying degrees in each patient. The estimated incidence of the syndrome ranges from 1 in 3500 to 5600 live births with a male-to-female ratio of approximately 3:2.[1]
Characteristic clinical findings of the syndrome include epibulbar dermoid or lipodermoid (mostly bilateral); colobomas of the upper eyelid, iris, chorioidea, and retina; or other eye anomalies. Other anomalies include preauricular skin tags or blind fistulas; microtia, or other external ear malformations; and middle and internal ear anomalies. There usually is unilateral facial hypoplasia, prominent forehead, hypoplasia of the zygomatic area, and maxillary and mandibular hypoplasia. Unilateral macrostomia and vertebral column anomalies are also seen.[1]
There are other associated malformations other than the main deformities, such as cleft lip and/or palate, tongue cleft, unilateral tongue hypoplasia, and parotid gland aplasia. There may be anomalies of the ribs and extremities including, but not limited to, radial limb anomalies, clinodactyly, polydactyly, syndactyly, and rocker bottom feet. Congenital heart diseases may include septal defects, tetralogy of Fallot, transposition of great vessels, dextrocardia, and pulmonary arterial anomalies. Anomalies of the urogenital and gastrointestinal system and even larynx can be associated with the disorder. Various central nervous system anomalies such as encephalocele, microcephaly, agenesis of corpus callosum, and Arnold–Chiari malformations along with complex retardation of mental development have also been reported.
Anomalies of the lungs such as pulmonary hypoplasia, aplasia, or agenesis are also reported.[1]
Ipsilateral lung involvement is more common as compared to contralateral lung involvement.[7]
The differential diagnosis for Goldenhar syndrome is broad and includes other congenital anomalies such as CHARGE Syndrome, Parry Romberg Syndrome, Nager syndrome, Townes–Brocks syndrome, or Treacher–Collins Syndrome. The closest differential is Treacher–Collins syndrome, where the facial involvement is bilateral, in contrast to Goldenhar syndrome, where it is unilateral. Mutation in the TCOF1 gene on chromosome 5q 31–34 helps in the final diagnosis of Treacher–Collins Syndrome.[12,13]
The facial and external ear malformations usually require surgical correction, mainly for cosmetic purposes. The lung malformations can lead to respiratory distress in childhood as well as recurrent chest infections which require proper medical management.[11]
The patient in our case had no respiratory complaints and had presented to the hospital for management of cleft palate. However, the patient had a history of recurrent chest infections in childhood and had undergone a CT scan for the same, where a diagnosis of the left-sided pulmonary hypoplasia was made. He was given medical management for the infections with no further management for pulmonary hypoplasia.
CONCLUSION
Goldenhar syndrome is a complex developmental disorder associated with anomalies of other organ systems such as cardiac structural anomalies, anomalies of genitourinary system, and pulmonary aplasia or hypoplasia, referred to as the expanded Goldenhar complex. Therefore, these should be sought for in a patient presenting with features of this anomaly even in absence of related symptoms.
TEACHING POINTS
Goldenhar syndrome is a rare congenital condition due to defects in first and second branchial arches, which mainly affect the craniofacial structures and vertebrae.
When associated with other major organ system anomalies cardiac structural defects, renal agenesis, pulmonary agenesis, and vascular anomalies, it is called expanded Goldenhar syndrome.
Association of pulmonary anomalies with Goldenhar syndrome is rare, ipsilateral lung involvement being commoner than contralateral lung involvement.
Patients presenting with craniofacial abnormalities compatible with this syndrome should also be investigated for other systemic abnormalities, even if asymptomatic.
MCQs
-
Anomalies of which branchial arches are observed in Goldenhar syndrome?
2nd and 3rd
3rd and 4th
1st and 2nd
1st and 4th
Answer Key: c
-
Which of the following statements are true?
Goldenhar syndrome is a hereditary disorder
Ipsilateral lung involvement is commoner than contralateral lung involvement
Incidence is higher in females
Pulmonary aplasia has a rudimentary, blind ending bronchus
Answer Key: b
-
Which is the closest differential for Goldenhar syndrome?
Treacher–Collins syndrome
CHARGE syndrome
Parry–Romberg syndrome
Nager syndrome
Answer Key: a
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Goldenhar syndrome with various clinical manifestations. Cleft Palate Craniofac J. 2006;43:628-34.
- [CrossRef] [PubMed] [Google Scholar]
- The roentgenological aspects of Goldenhar's syndrome (oculoauriculovertebral dysplasia) Radiology. 1968;91:254-60.
- [CrossRef] [PubMed] [Google Scholar]
- A constellation of rare findings in a case of Goldenhar syndrome. Case Rep Pediatr. 2017;2017:3529093.
- [CrossRef] [PubMed] [Google Scholar]
- Caudal regression and encephalocele: Rare manifestations of expanded Goldenhar complex. Case Rep Pediatr. 2017;2017:4396142.
- [CrossRef] [PubMed] [Google Scholar]
- Pulmonary hypoplasia in a newborn with Goldenhar syndrome. J Pediatr. 2010;156:161.
- [CrossRef] [PubMed] [Google Scholar]
- Right pulmonary agenesis with ipsilateral microtia: A new laterality association or part of the oculoauriculovertebral spectrum? Prenat Diagn. 2002;22:1053-4.
- [CrossRef] [PubMed] [Google Scholar]
- Pulmonary agenesis: A predictor of ipsilateral malformations. Am J Med Genet. 1997;70:391-8.
- [CrossRef] [Google Scholar]
- Goldenhar syndrome: A new case expanding the phenotype by costal agenesis and pulmonary hypoplasia. Eur Rev Med Pharmacol Sci. 2012;16:1307-8.
- [Google Scholar]
- Goldenhar syndrome with contralateral pulmonary aplasia: A rare association. J Radiol Case Rep. 2016;10:35-40.
- [CrossRef] [PubMed] [Google Scholar]
- Goldenhar syndrome: A case report with review. Int J Clin Pediatr Dent. 2016;9:278-80.
- [CrossRef] [PubMed] [Google Scholar]
- Oculo auriculo vertebral dysplasia Goldenhar syndrome. IP Int J Ocular Oncol Oculoplast. 2022;8:80-2.
- [CrossRef] [Google Scholar]




