

Translate this page into:
Coronary artery anomalies: Rare coronary artery anomalies detected on coronary computed tomography angiography

*Corresponding author: Angshumi Deka, Department of Radiodiagnosis, Assam Medical College and Hospital, Dibrugarh, Assam, India. angshumi681@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Deka A, Nath L, Kalita HC. Coronary artery anomalies: Rare coronary artery anomalies detected on coronary computed tomography angiography. Case Rep Clin Radiol. doi: 10.25259/CRCR_6_2025
Abstract
Coronary artery anomalies are rare congenital cardiovascular defects that can present in various ways depending on the origin, course, and termination of the abnormal coronary artery. It is sometimes detected incidentally during procedures such as coronary angiography or autopsies. Most of the time, they are often asymptomatic, but some may experience angina with congestive heart failure, myocardial infarction, cardiomyopathy, ventricular aneurysms, or sudden cardiac death. In this discussion, we provide a concise overview of three specific cases: One involving a common origin of the left coronary artery and right coronary artery (RCA) from the right coronary sinus, another congenital absence of RCA, and a third case involving a high origin of RCA which were diagnosed by coronary computed tomography angiography.
Keywords
Computed tomography coronary angiography
Coronary artery anomalies
Cardiac imaging

INTRODUCTION
Coronary artery anomalies (CAAs) refer to a group of congenital anomalies that are associated with the aberrant origin or path of any of three main epicardial arteries.[1] Individuals having any of those anomalies are mostly asymptomatic until discovered incidentally and rarely may present with life-threatening situation ranging from congenital heart failure, arrhythmia, myocardial infarction, or sudden cardiac death. These are very rare anomalies and are seen in approximately 1–2% of general population.[2]
CASE SERIES
Case 1
A 31-year-old female presented with a history of palpitation on and off and mild chest pain on exertion for the past 1 month. Electrocardiogram (ECG) was done which revealed arrhythmia. Computed tomography (CT) coronary angiography was advised which revealed a common origin of both left and right coronary circulation from the right coronary sinus [Figure 1]. The left-sided circulation was originating from the right coronary sinus and is noted to take a dip before traversing through the interventricular septum (transeptal course).
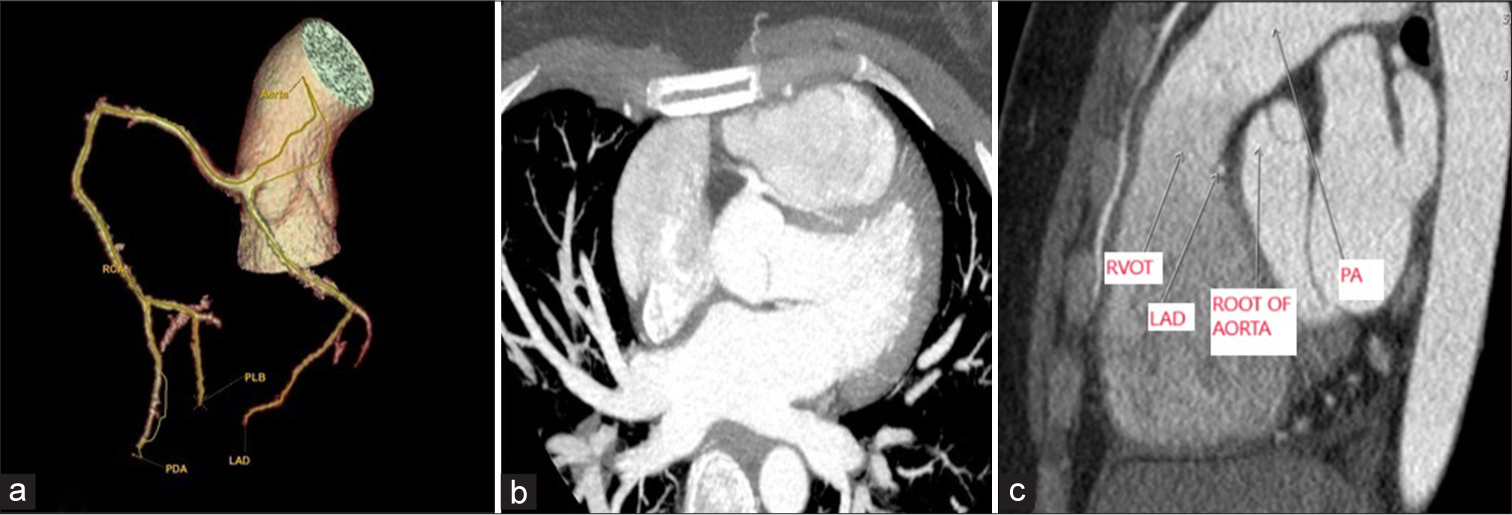
- Computed tomography angiography examination of coronary arteries (a) 3-D reconstruction of coronary arteries (b) Axial maximum intensity projection image shows the common origin of LCA and RCA from the right coronary sinus (c) sagittal images shows origin of LCA from the right coronary sinus and is following a transeptal course. RCA: Right coronary artery, LCA: Left coronary artery, LAD: Left anterior descending artery, RVOT: Right ventricular outflow tract, PA: Pulmonary artery.
Case 2
A 49-year-old man presented with a history of chest pain and difficulty in breathing that aggravated on exertion. ECG showed non-specific ST-T changes. Cardiac enzymes were within normal limits. On invasive coronary angiography, few plaques in the left anterior descending (LAD) were noted without causing any significant luminal narrowing. However, the physician could not find the right coronary sinus. Suspecting a congenital abnormality, he was further advised to undergo CT coronary angiography which revealed an absent right-sided coronary circulation [Figure 2]. There was only left-sided coronary circulation which was supplying both the halves. The left circumflex (LCx) gave posterolateral ventricular branch (PLVB) and posterior descending artery (PDA) branches which followed its usual course.
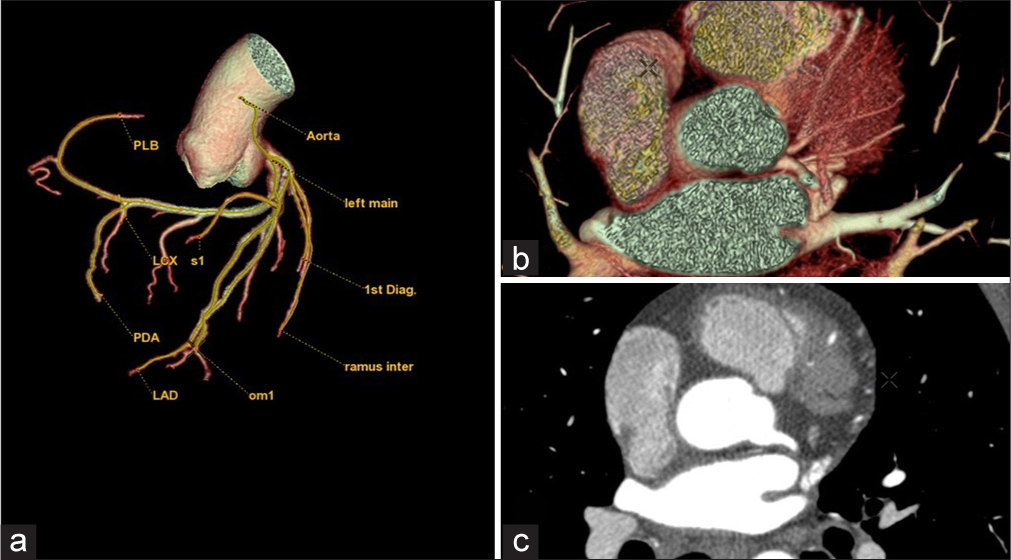
- Computed tomography angiography examination of coronary arteries (a) 3-D reconstruction of coronary arteries, (b) axial volume rendering image, (c) maximum intensity projection axial computed tomography images showing absence of right coronary artery and presence of only left coronary circulation which is supplying the entire heart. LMA: Left main artery, LCA: Left coronary artery, PA: Pulmonary artery, RCS: Right coronary sinus.
Case 3
A 59-year-old man who had a known case of hypertension and type 2 diabetes mellitus on irregular medication presented to the cardiology department of our hospital with complaints of chest pain for 1 month which was gradually worsening and was radiating to the left shoulder and back. Invasive coronary angiography revealed marked narrowing of the LAD in the distal part (approximately 90%). However, the RCA could not be localized in invasive coronary angiography. CT coronary angiography was done for better localization of RCA. CT coronary angiography revealed that the origin of RCA was higher than its usual location approximately at distance of 1.8 cm from sino-tubular junction on the right side [Figure 3]. Distal to that was a normal RCA route and distribution without any evidence of vessel injury, stenosis, or plaque within.
![Computed tomography angiography examination of coronary arteries (a) 3D reconstruction of coronary arteries showing high take off RCA on the right side with associated significant stenosis in LAD (b) anterior oblique volume rendering images showing RCA arising high above the right coronary sinus (white straight line (3) approx. 1.8 cm from sinotubular junction) and origin of LCA from usual left coronary sinus. LMA: Left main artery, RCA: Right coronary artery, PA: Pulmonary artery [white arrow (1) aorta, white arrow (2) point from where RCA is arising from the aorta].](/content/152/2025/0/1/img/CRCR-6-2025-g003.png)
- Computed tomography angiography examination of coronary arteries (a) 3D reconstruction of coronary arteries showing high take off RCA on the right side with associated significant stenosis in LAD (b) anterior oblique volume rendering images showing RCA arising high above the right coronary sinus (white straight line (3) approx. 1.8 cm from sinotubular junction) and origin of LCA from usual left coronary sinus. LMA: Left main artery, RCA: Right coronary artery, PA: Pulmonary artery [white arrow (1) aorta, white arrow (2) point from where RCA is arising from the aorta].
DISCUSSION
In Case 1, an atypical left coronary artery (LCA) originating from the right coronary sinus is extremely uncommon, described to occur in just 0.02–0.05% of cases in angiographic studies.[3] Although the artery originates from an ectopic source, the critical issue lies in the path that the aberrant coronary artery follows to reach its perfusion territory.[4]
There are five possible pathways described as follows: (1) Prepulmonic, (2) Retroaortic, (3) Transseptal, (4) Interarterial, and (5) Retrocardiac.
In Case 2, congenital absence of the right coronary artery (RCA) is a specific form of severe congenital anomaly that was initially identified in 1948 by White and Edwards.[5] Autopsy findings indicate that single coronary arteries are extremely uncommon, occurring in about 0.014–0.066% of cases.[6] In general, the RCA supplies the sinoatrial (SA) and atrioventricular (AV) nodes. Provided that there is just one LCA that supplies the SA and AV nodes, together with the other cardiac structures, the SA or AV node may degenerate early due to insufficient blood supply.[7] The excessively used single LCA can undergo dilation, fistula formation, and compression of adjacent structures or branches, leading to ischemia and early endothelial damage, therefore contributing to the development of early atherosclerosis.[8]
In Case 3, RCA with a high take-off that is exceedingly uncommon often presents as incidental findings on imaging modalities or during cardiac surgery for another indication.[9] The reported incidence ranges from 0.019 to 0.17%.[10] High take-off suggests that the RCA or left main coronary artery (LMCA) originates at a point more than 5 mm above the sino-tubular junction, from the ascending aorta.[3,4] It is more frequently observed in conjunction with the RCA, with a reported prevalence of bilateral high take-off of up to 6%.[11] The relative risk that the anomalous RCA entails is indicated by its sites and courses.[12,13] They are more susceptible to unforeseen injury.[11] This type of anomaly can be completely missed or misdiagnosed.
CONCLUSION
Our case series underscores the critical role of CT coronary angiography in the early and accurate diagnosis of CAAs. These anomalies, while often asymptomatic, can have significant implications for patient management and outcomes. By highlighting a diverse range of presentations and providing insights into their clinical relevance, this report aims to enhance awareness and improve diagnostic accuracy. Early detection through advanced imaging techniques like CT coronary angiography can facilitate timely intervention and personalized care, ultimately contributing to better patient outcomes.
TEACHING POINTS
The case series highlights the importance of CT coronary angiography in detecting rare coronary anomalies that may be missed or misdiagnosed by invasive coronary angiography
While some anomalies are benign, others can lead to ischemia, arrhythmias, endothelial damage, and early atherosclerosis, emphasizing the need for individualized patient management
Since these anomalies are rare, increasing awareness among healthcare professionals can improve diagnostic accuracy, guide treatment decisions, and potentially prevent adverse outcomes.
MCQs
-
Which of the following is NOT a possible course for an anomalous coronary artery?
Prepulmonic
Retroaortic
Intercostal
Transseptal
Answer Key: c
-
Which coronary artery supplies the RCA territory in cases of congenital absence of RCA?
LAD artery
LCx artery
PDA from the RCA
None, as the right side remains unsupplied
Answer Key: b
-
A high take-off of the RCA is defined as its origin more than how many millimeters above the sino-tubular junction?
2 mm
5 mm
10 mm
20 mm
Answer Key: b
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Anomalies of coronary artery origin: Evaluation on multidetector CT angiography. Clin Imaging. 2019;57:87-98.
- [CrossRef] [PubMed] [Google Scholar]
- Coronary artery anomalies overview: The normal and the abnormal. World J Radiol. 2016;8:537-55.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiac imaging: part 2, normal, variant, and anomalous configurations of the coronary vasculature. AJR Am J Roentgenol. 2011;197:816-26.
- [CrossRef] [PubMed] [Google Scholar]
- Anomalies of the coronary arteries; Report of four cases. Arch Pathol (Chic). 1948;45:766-71.
- [Google Scholar]
- Isolated single coronary artery: Diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39-47.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital absence of the right coronary artery: A case report and literature review. Medicine (Baltimore). 2018;97:e0187.
- [CrossRef] [PubMed] [Google Scholar]
- A rare anatomical variant: congenital absence of the right coronary artery with left circumflex artery supplying the right coronary artery (RCA) territory. Am J Case Rep. 2021;22:e932248.
- [CrossRef] [Google Scholar]
- An incidental encounter of a rare high take-off right coronary artery: A case report. Medicine (Baltimore). 2017;96:e8614.
- [CrossRef] [PubMed] [Google Scholar]
- Right coronary artery with high Takeoff. Ann Thorac Surg. 2007;83:1867-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pathology of coronary disease. Semin Roentgenol. 1972;7:376-94.
- [CrossRef] [PubMed] [Google Scholar]
- Acute coronary syndrome due to high aortocoronary junction of the right coronary artery: The value of multislice CT. Int J Cardiol. 2008;123:e59-61.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital coronary artery anomalies in adults: Non-invasive assessment with multidetector CT. Br J Radiol. 2009;82:254-61.
- [CrossRef] [PubMed] [Google Scholar]




