

Translate this page into:
A rare cause of esophageal dysphagia due to dilatation of azygos vein

*Corresponding author: Ajeya Asarkar, Department of Radiology, Grant Government Medical College and JJ Hospital, Mumbai, Maharashtra, India. asarkar.ajeya@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh SS, Ghatge SB, Asarkar A, Bagul RK. A rare cause of esophageal dysphagia due to dilatation of azygos vein. Case Rep Clin Radiol. doi: 10.25259/CRCR_91_2024
Abstract
Dysphagia is defined as an inability to swallow or difficulty in the passage of food from the mouth to the stomach due to functional or mechanical obstruction of the luminal organ, including the oropharynx, esophagus, or gastric cardiac. The azygos vein (AV) begins as the confluence of the upper lumbar and right subcostal veins before it enters the thoracic cavity. It runs closely alongside the esophagus and thoracic duct through the posterior mediastinum, and it receives contributions from the left-sided hemiazygos and accessory hemiazygos veins. The AV arches over the esophagus anteriorly before draining into the superior vena cava. Due to its close anatomical proximity to the esophagus, the AV can potentially cause dysphagia if significant pathology is present. The etiologies of esophageal dysphagia can be divided into structural and motor disorders. The structural disease can be further subdivided into intrinsic and extrinsic causes. External vascular compression is a rare but crucial consideration in diagnosing dysphagia, often linked to arterial abnormalities. Among these, an aberrant right subclavian artery – known as arterial lusoria – is the most common. In contrast, venous abnormalities are even less likely to cause a mass effect due to their relatively soft, compressible structure. Azygos vein aneurysms are uncommon and infrequently diagnosed.
Keywords
Azygos vein aneurysm
Dysphagia
Barium study
Computed tomography pulmonary angiography
Azygos vein

INTRODUCTION
Dysphagia resulting from vascular abnormalities is a rare condition, with a prevalence of <1%, characterized by compression of the esophagus from abnormal intrathoracic vascular structures. As of now, and to the best of our knowledge, only 57 cases of azygos vein aneurysm (AVA) have been reported in the literature, and probably the first case in India. William Osler first identified an AVA during an autopsy in 1915, and William Walker later described it in 1963. Typically, the normal azygos vein (AV) measures ≤1 cm in diameter, though its size can vary depending on anatomical location and volume status. While there is no established diagnostic size criterion for AVA, some sources suggest that a focal dilation of ≥2.5 cm at the body of the AV and ≥3.75 cm at the AV arch could be indicative.[1,2]
Here, we report a rare case of esophageal dysphagia due to AV focal dilatation in a 60-year-old male.
CASE REPORT
A 60-year-old male came to the hospital with complaints of difficulty in swallowing, blood in sputum, breathlessness on exertion, generalized weakness, and fever on and off for 1 month.
The patient had a history of pulmonary tuberculosis (PTB) twice and took a complete anti-tubercular medicine course. The patient denied a history of alcoholism.
The imaging workup was done. Barium swallow showed that there is focal dilatation with extrinsic compression in the mid-esophageal region [Figure 1]. Computed tomography (CT) pulmonary angiography showed a dilated AV with the largest diameter of 13 mm and length of 5.1 cm, which causes extrinsic compression to the posterolateral aspect of the midesophageal region [Figure 2].
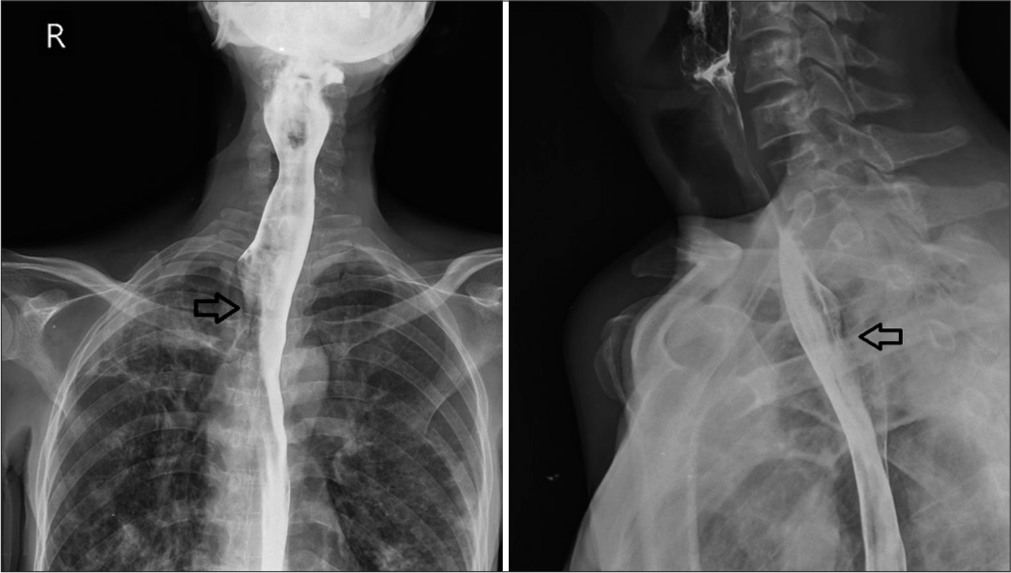
- (a) Barium swallow (anterior posterior view): Focal dilatation with extrinsic compression in the mid esophageal region (black arrow). (b) Barium swallow in lateral view (black arrow).
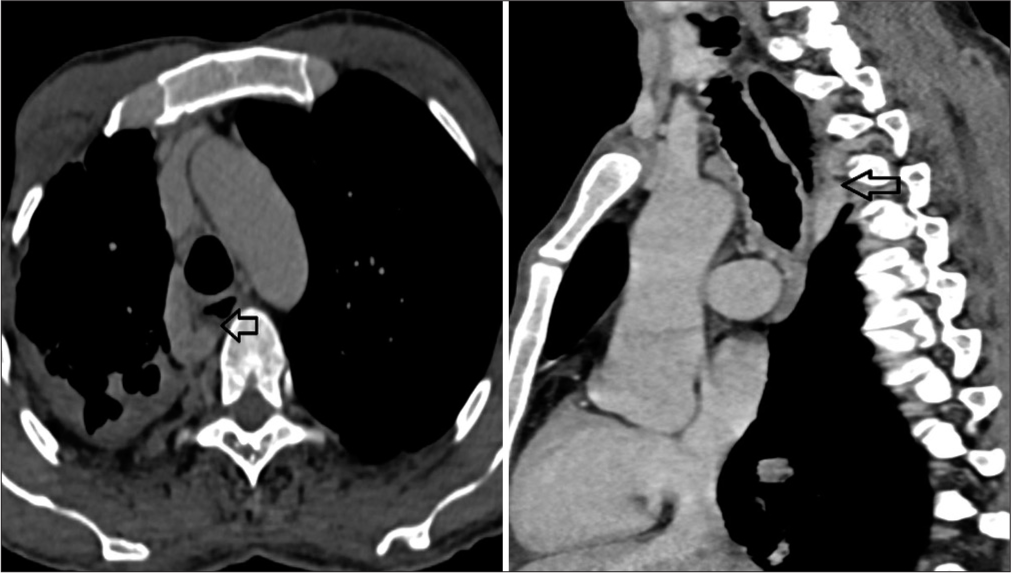
- (a) Computed tomography (CT) pulmonary angiography (axial view) showed a dilated azygos vein with the largest diameter of 13 mm, which causes extrinsic compression to the posterolateral aspect of the mid-esophageal region (black arrow). (b) CT pulmonary angiography (black arrow).
Esophagogastroduodenoscopy revealing no evidence of luminal lesions with mild portal hypertensive gastropathy. The final diagnosis was dysphagia due to extrinsic compression of dilated AVA. The patient was managed conservatively and given discharge after 12 days.
DISCUSSION
The AV originates from the confluence of the upper lumbar and right subcostal veins before it enters the thorax. It travels close to the esophagus and thoracic duct through the posterior mediastinum, receiving blood from the hemiazygos vein and the accessory hemiazygos vein. At the T8–T9 level, the hemiazygos vein drains into the AV, which then empties into the superior vena cava (SVC) [Figure 3].[3] Due to its anterior arch over the esophagus before it terminates in the SVC, any dilation or aneurysm of the AV can potentially cause symptoms such as dysphagia, as observed in this patient.
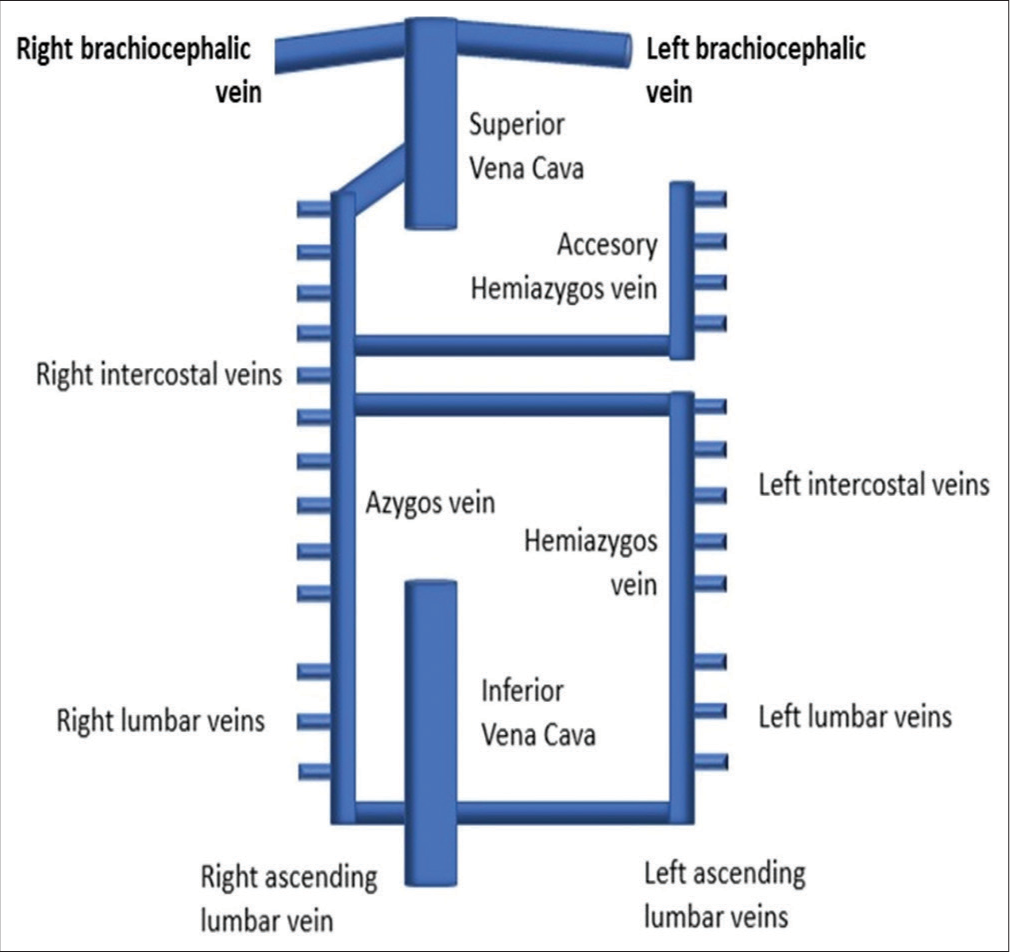
- Schematic diagram of azygos vein anatomy.
Persistent and recurrent difficulty swallowing solid foods, despite normal findings on endoscopy, should prompt clinicians to consider underlying causes such as motility disorders or external compression by intrathoracic structures in appropriate clinical contexts. Acquired abnormalities of the AV can occur due to hemodynamic changes, leading to enlargement or the presence of lesions, which result in compression.[4]
Differential diagnoses for vascular causes of dysphagia are shown in Table 1.
| 1) CHF 2) Constrictive pericarditis 3) IVC obstruction 4) Portal hypertension 5) SVC obstruction (distal to azygos entry) 6) Congenital SVC interruption (distal to azygos entry) 7) Congenital IVC interruption 8) Tricuspid insufficiency 9) Right ventricular strain |
CHF: Congestive heart failure, SVC: Superior vena cava, IVC: Inferior vena cava
In dysphagia, clinical presentations vary, emphasizing the need for careful evaluation and differentiation from other causes of dysphagia to rule out other differentials. Diagnosis typically involves imaging studies such as CT scans or barium swallow tests to visualize the anatomical relationship and confirm compression, which helps to narrow down the diagnosis.
Complications such as mass effect can occur due to AVA or AV dilation; yet there is no universally accepted approach for management. Typically, asymptomatic patients are managed conservatively with regular monitoring. For those with symptoms, treatment focuses on preventing thromboembolism and rupture of the aneurysm, as well as alleviating symptoms. In this case, the initial treatment involved careful observation and symptom management. Surgical interventions, including resection with or without venous bypass, have also proven successful.
Although rare, vascular compression of the esophagus can cause dysphagia and may improve with intervention, underscoring the need for a high level of clinical suspicion in making this diagnosis.
Management strategies may begin with conservative approaches such as dietary modifications to ease swallowing. In cases where symptoms persist or worsen, consideration of surgical intervention or interventional procedures becomes necessary to alleviate the compression and improve swallowing function.[5]
CONCLUSION
This case highlights one of the rare causes of dysphagia due to AVA. Cross-sectional imaging, like a CT scan, will be crucial for the diagnosis of extrinsic compression of the esophagus. It is advisable to consider the rare causes of extrinsic compression of the esophagus while reporting the cross-sectional imaging and barium esophagogram. Endoscopy is likely to be normal in such cases. Diagnostic criteria for AVA in both symptomatic and asymptomatic need to be validated by meta-analysis of reported cases.
TEACHING POINTS
When diagnosing dysphagia, it is crucial to consider vascular compression, especially if endoscopic findings are normal. Imaging studies such as CT scans and barium swallow tests are essential for visualizing the anatomical relationship and assessing for any compression caused by an enlarged azygos vein.
Patient education is important, emphasizing the understanding of the condition, treatment options, and the necessity of follow-up to monitor progress and address any recurrence effectively.
MCQs
-
What is the primary anatomical relationship of the azygos vein in the thoracic cavity?
It runs parallel to the esophagus and thoracic duct through the anterior mediastinum.
It originates from the left subcostal vein and travels posterior to the esophagus.
It travels close to the esophagus and thoracic duct through the posterior mediastinum.
It drains directly into the left atrium of the heart.
Answer Key: c
-
When diagnosing vascular causes of dysphagia, which imaging studies are typically utilized?
Barium swallow test and CT scan
X-ray and ultrasound
Magnetic resonance imaging and positron emission tomography scan
Endoscopy and echocardiogram
Answer Key: a
-
What is a common conservative management strategy for patients with asymptomatic azygos vein abnormalities?
Immediate surgical resection
Chemotherapy
Radiation therapy
Regular monitoring with observation
Answer Key: d
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Azygos vein aneurysm mimicking a mediastinal mass. In Vivo. 2020;34:2135-40.
- [CrossRef] [Google Scholar]
- Multifactorial dysphagia: Azygos vein aneurysm (Ava) and esophagogastric junction outflow obstruction (EGJOO) Int J Surg Case Rep. 2021;83:106017.
- [CrossRef] [Google Scholar]
- The azygos vein pathway: An overview from anatomical variations to pathological changes. Insights Imaging. 2014;5:619-28.
- [CrossRef] [Google Scholar]
- Clinical significance of azygos vein enlargement: Radiographic recognition and etiologic analysis. Clin Imaging. 1999;23:236-41.
- [CrossRef] [Google Scholar]
- S2871 dilated azygous vein secondary to inferior vena cava atresia as a rare cause of dysphagia. Am J Gastroenterol. 2023;118:S1947-8.
- [CrossRef] [Google Scholar]




